
Laparoscopic Paraesophageal Hernia Repair
Main Text
Table of Contents
Surgical repair should be considered in all symptomatic paraesophageal hernias. Laparoscopic repair is considered the gold standard with a quicker recovery and lower morbidity and mortality compared to open repairs. The patient in this case presented with worsening dysphagia to solids and dyspnea in the setting of an enlarging paraesophageal hernia with a component of organoaxial volvulus. She underwent a laparoscopic paraesophageal hernia repair with a Toupet fundoplication and posterior gastropexy. The patient exhibited subjective improvement in her dysphagia to solids and dyspnea with exertion as well as an objective improvement in her pulmonary function tests postoperatively.
A true type II paraesophageal hernia is characterized by herniation of the stomach into the posterior mediastinum while maintaining normal positioning of the LES. Mixed hernias (type III) and giant hernias (type IV) are often described as paraesophageal hernias as well. Many of these patients are elderly and are often asymptomatic with their hiatal hernias discovered incidentally on imaging. Symptoms may be caused by gastric outlet obstruction (eg, postprandial pain and early satiety), gastroesophageal reflux, or mechanical trauma to the gastric mucosa (eg, occult blood loss). All symptomatic patients who are good operative candidates should have their paraesophageal hernias repaired. Asymptomatic patients should be observed whereas minimally symptomatic patients who are higher risk surgical candidates require thoughtful decision making before being recommended surgical repair.
The patient is an 85-year-old woman with a history of GERD and long-standing dysphagia that had recently progressed with associated weight loss. She endorsed significant trouble swallowing solid foods and occasionally even liquids. She also endorsed a history of worsening dyspnea, particularly with activity. She had a known hiatal hernia that was documented to have enlarged on a recent barium swallow. The most recent barium swallow demonstrated weak esophageal peristalsis with a corkscrew shaped esophagus and a large hiatal hernia with organoaxial volvulus. An upper endoscopy confirmed the presence of these anatomical findings as well as the presence of Cameron ulcers. Esophageal motility disclosed a normal LES resting pressure and incomplete LES relaxation on 5 of 11 swallows. Finally, a 24-hour pH impedance study on PPI therapy showed mild reflux but no correlation with symptoms. Her dysphagia did not improve with Botox injections.
On examination, the patient exhibited no abnormal cardiopulmonary findings. She had no prior history of abdominal surgery, and her abdominal exam was normal. In the case of this patient, she had no significant cardiac history or history of arrhythmias and a preoperative ECG was unremarkable. Pulmonary function testing was performed given her worsening dyspnea. She was found to have a moderate restrictive defect without significant improvement with albuterol administration. Her worsening dyspnea was thought to be related to her enlarging paraesophageal hernia.
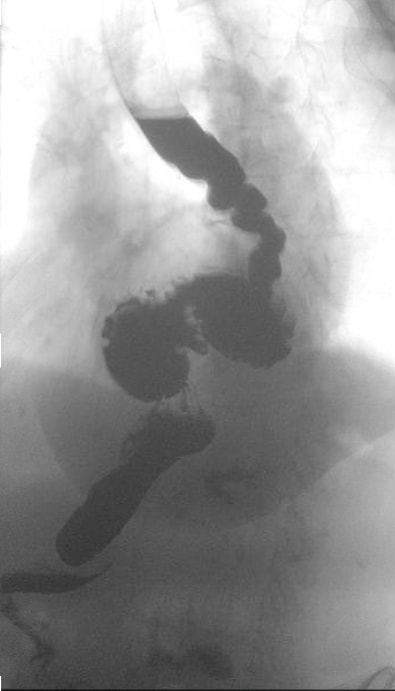 Figure 1a. Upper GI swallow study demonstrating a corkscrew esophagus and paraesophageal hernia with organoaxial volvulus.
Figure 1a. Upper GI swallow study demonstrating a corkscrew esophagus and paraesophageal hernia with organoaxial volvulus. 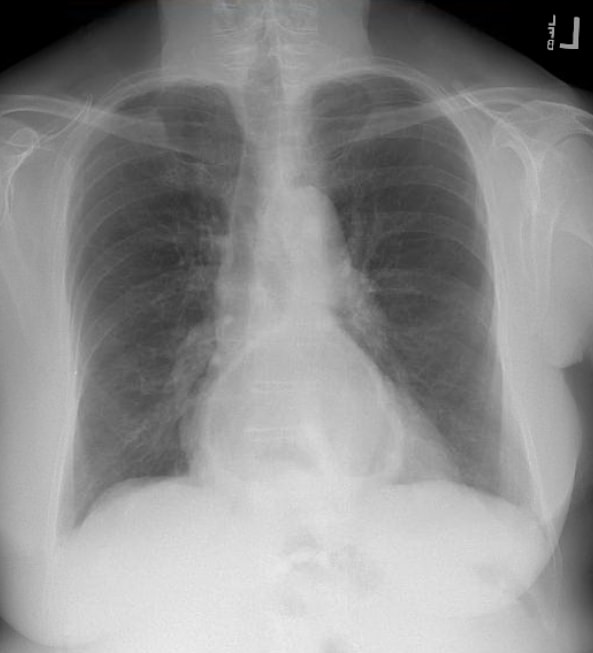 Fig. 1b. CXR showing a posterior air-fluid level consistent with a large hiatal hernia.
Fig. 1b. CXR showing a posterior air-fluid level consistent with a large hiatal hernia.Initial diagnosis is most often made incidentally either on a chest radiograph demonstrating an air-fluid level in the mediastinum posterior to the heart, on a CT scan ordered for other symptoms, or during an upper GI endoscopy. For surgical candidates, evaluation consists of assessing the patient’s overall health status as well as defining the anatomy. CT provides the benefit of three-dimensional anatomy of the hernia. Patients who have a component of preoperative dysphagia should undergo esophageal manometry prior to any fundoplication. An upper endoscopy must be performed preoperatively to exclude concomitant disease such as Barrett’s esophagus, peptic ulcer disease, neoplasms, or other pathology.
Paraesophageal hernias are a disease of the elderly with a median age of presentation between 60–70 years old. Paraesophageal hernias represent a small subset of hiatal hernias (5–10%) and can range from asymptomatic to life-threatening complications. Most of these hernias are asymptomatic or minimally symptomatic, but a small subset of patients can progress to developing acute symptoms, estimated to be about 1% risk of symptom progression per year.1
For symptomatic patients, there are three primary approaches: 1) an open transabdominal approach through an upper midline laparotomy, 2) an open transthoracic approach through a left thoracotomy, and 3) a laparoscopic approach. Laparoscopic repair is considered the standard of care with lower overall morbidity and mortality compared to open repair. The principles of the repair are the same irrespective of access: reduction of intra-abdominal contents, dissection and removal of the hernia sac, mobilization and tension-free return of the gastroesophageal junction into the abdomen, and repair of the diaphragmatic defect. The addition of an anti-reflux procedure or fundoplication should be considered in all patients to minimize post-op reflux symptoms. If dysmotility is present, a partial fundoplication is preferred.
Surgical repair is indicated to relieve symptoms. In patients with minimal symptoms, the risk of complications from surgery must be weighed against the lifetime risk of strangulation or progression of symptoms. This risk is about 1–2% annually.
Our patient presented with reflux and weight loss in the setting of progressive dysphagia. Her evaluation disclosed concomitant esophageal dysmotility and gastroesophageal junction obstruction (as well as worsening dyspnea) thought to be due to her large paraesophageal hernia. We elected to proceed with a laparoscopic paraesophageal hernia repair with a partial fundoplication, expecting her dysphagia to improve with restoration of more normal anatomy.
The vast majority of paraesophageal hernias can be repaired laparoscopically. However, surgeons performing these procedures must be prepared for difficult cases wherein esophageal lengthening or adjunctive techniques for crural repair are needed. The use of mesh to reinforce repairs is controversial with no high-level evidence to suggest that absorbable mesh improves long-term outcomes.
Patient factors such as age, obesity, hepatomegaly, or extensive prior abdominal surgery may alter surgical plans. Prior to proceeding with repair, it is important to weigh the morbidity and mortality of elective repair compared to the lifetime risk of volvulus and need for an emergent surgery and its associated risks.
Generally, these patients tend to be elderly and require a perioperative cardiopulmonary risk assessment and testing on an individual basis. Studies have shown that patients aged 80–90 undergoing both elective and emergent hiatal hernia repair face significantly higher risks of death and complications compared to those aged 65–79, even after accounting for comorbidities. This suggests that delaying elective repair until the eighth decade of life increases the risk of poor outcomes. Additionally, while age alone may not always predict mortality, emergent operations significantly increase the risk. Age over 72 and high frailty double the odds of morbidity after elective repair. These findings highlight the importance of timely elective repair to improve outcomes in elderly patients.21
Obesity is frequently associated with hiatal hernias and is known to elevate the risk of recurrence following hiatal hernia repair. Therefore, it would be beneficial for patients with higher BMIs to lose weight prior to hiatal hernia repair in order to avoid recurrence. Given the rise of new medical weight loss treatments, future research should explore the BMI levels at which patients might benefit from lifestyle changes, medical interventions, or surgical weight loss before undergoing hiatal hernia repair.20 In our experience the mentioned threshold is 35 kg/m2.
The management of asymptomatic hiatal hernias, as outlined in the SAGES Guidelines for the Surgical Treatment of Hiatal Hernias, is challenging due to limited evidence. The panel formulated a recommendation based on expert opinion, which emphasizes the importance of confirming true asymptomatic status, as many patients may have non-gastrointestinal symptoms linked to the hernia, such as shortness of breath, exercise intolerance, or abnormal echocardiogram findings. For those confirmed to be asymptomatic, the decision between surgical repair and continued surveillance should involve a detailed discussion of potential risks and benefits. Surgery might prevent complications like reflux disease progression or micro-aspiration. However, the evidence supporting these interventions is not robust, making patient involvement in decision-making crucial.
The potential for an asymptomatic hiatal hernia to progress to an acute gastric volvulus is a significant concern, yet there is insufficient data to identify which patients are at higher risk. Studies comparing elective hernia repair to watchful waiting have produced mixed results, with some favoring surveillance and others suggesting improved quality of life with surgery. Given this uncertainty, a watchful waiting approach is reasonable if the patient understands and accepts the associated risks. Shared decision-making and thorough discussions at each evaluation stage are essential for achieving the best outcomes.20
Hiatal hernia was first described in the 16th century and most notably published by Bowditch in 1853 in a review of post-mortem findings from previously published cases.1 With the advent of radiography and x-rays, hiatal hernias were first diagnosed in living patients in the early 20th century. It was also at this time that Akerlund described paraesophageal hernias and attempted to classify hiatal hernias.1 Soresi described the first transabdominal approach to repair in 1919 while the earliest series of elective repair was described by Harrington in 1928 at the Mayo Clinic.1 In 1950, Sweet first published his transthoracic approach to paraesophageal hernia repair at the Massachusetts General Hospital.1 With the advent of minimally invasive surgery, the first laparoscopic paraesophageal hernia repair was described in 1992 and is now often described as the standard of care. Figure 2 demonstrates the common port placement utilized.

Figure 2. Port placement sites for laparoscopic paraesophageal hernia repair.
Hiatal hernias occur when a portion of the normally intra-abdominal stomach prolapses into the posterior mediastinum through the diaphragmatic hiatus.2 The most common type of hiatal hernia is the type I or sliding hernia, in which the gastroesophageal junction (GEJ) migrates through the diaphragmatic hiatus, thus displacing the location of the lower esophageal sphincter (LES) and exposing the LES to negative intrathoracic pressure. This combination of reduced pressure in the LES and displacement of its normal anatomical position leads to disruption of the anti-reflux mechanism of the LES.2 A true paraesophageal hernia (type II), while rare, is described as an upward herniation of the fundus of the stomach with a normally positioned GEJ. The term paraesophageal hernias is also used to describe both type III hiatal hernias where both the GEJ and fundus of the stomach are intrathoracic and type IV or giant paraesophageal hernias where additional intra-abdominal organs are herniated through the diaphragmatic hiatus as well.
Most hiatal hernias are seen in the elderly with the suggested pathophysiology that increasing age predisposes to changes and weakening of the crural muscles and surrounding connective tissue that make up the hiatal hernia margins. The large majority are asymptomatic and discovered incidentally on imaging or upper endoscopy. However, symptoms can range from mild in severity, such as gastroesophageal reflux and vague epigastric pain, to more severe, such as bleeding with chronic anemia, impaired pulmonary function and life-threatening organoaxial volvulus.
Historically, there was a general agreement amongst surgeons that all symptomatic paraesophageal hernias should be repaired in patients without substantial operative risk. The repair of asymptomatic paraesophageal hernias is more controversial. Initially, surgical repair, regardless of symptoms, was favored due to the fear of life-threatening organoaxial volvulus, once estimated to have a mortality as high as 30% by Skinner and Belsey in 1967 and 56% by Hill in 1973.3,4 These numbers overestimate the true mortality of emergency surgery for gastric volvulus. An analysis of the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database demonstrated that paraesophageal hernia repairs performed in an emergency setting had a mortality of 8%, which was 10 times greater than the elective surgery group but far lower than previous estimates.5 With multivariable analysis controlling for patient and disease-related factors, the study also found that emergent surgery did not independently predict mortality. They concluded that increased mortality was more a function of severe preoperative comorbidities and poor functional status that would have otherwise excluded patients from elective repair.5 Ballian et al developed a predictive model for perioperative mortality, identifying non-elective operation, age 80 or greater, history of pulmonary disease, and history of congestive heart failure as variables that carry increased risk for perioperative mortality.6
Stylopoulos et al challenged the idea that asymptomatic PEH should be repaired to prevent life threatening complications by championing a more conservative approach. Using a Markov Monte Carlo analytic model, the authors tracked a hypothetical cohort of asymptomatic and minimally symptomatic patients and outcomes associated with elective laparoscopic repair and a conservative watchful waiting strategy. If symptom progression is constant and age dependent, then the risk of developing life-threatening symptoms for a 65-year-old patient is 18% or 1.1% per year.7 Assuming a mortality of emergency surgery of 5.4% from pooled data and the Nationwide Inpatient Sample (NIS) database, then the overall risk of death from watchful waiting was approximately 1%, similar to the pooled estimate of 1.38% for elective laparoscopic repair.7 Watchful waiting was the optimal treatment strategy for 83% of patients in the analysis.
Although paraesophageal hernia were initially repaired via an open transabdominal or transthoracic approach, laparoscopic repair has now emerged as the standard for care. Benefits of laparoscopic PEH repair include less postoperative pain, shorter length of stay, faster recovery, and improvement in quality of life.8 Patients undergoing laparoscopic paraesophageal hernia repair also have fewer overall complications, less need for intensive care unit care, and fewer 30-day readmissions in addition to the aforementioned benefits.9 Mungo et al examined the NSQIP database including 8186 patients who had undergone a PEH (laparoscopic vs open) and discovered an overall 30-day mortality of 0.92% (2.6% open, 0.5% laparoscopic) with significantly lower morbidity in laparoscopic repair, even after adjusted for emergent cases.10 Fullem et al echoed these findings after examining the NIS database (23,514 patients) and concluded that laparoscopic repair is associated with lower mortality compared to an open approach in uncomplicated PEH repair (0.57% vs 1.34%).11
The addition of a fundoplication following repair helps minimize post-op reflux symptoms. Even though reduction of the hernia and mobilization of the stomach to a normal anatomic position alone significantly reduces reflux symptoms (54.6% to 18.2%, P = 0.011), the addition of a fundoplication shows an even more substantial reduction in these symptoms (67.7% to 5.4%, P < 0.001).12 Fundoplication has no impact on reducing hernia recurrence even though it has been postulated that the wrap helps anchor the stomach within the abdomen. Fundoplication should be avoided in patients with preoperative dysphagia or abnormal manometry suggestive of esophageal dysmotility.
Paraesophageal hernia repair provides nearly two-thirds of patients with complete symptom relief and significantly improves quality of life.13 Lidor et al found significant improvement in quality of life scores following surgical repair. All individual symptoms improved significantly except early satiety, nausea, pain with swallowing, and bloating/gas at 36 months.14 These symptoms still demonstrated improvement though they were not statistically significant. Almost all patients with postoperative heartburn symptoms are easily controlled with PPI therapy and very rarely require reoperation.
The downside of laparoscopic repair compared to an open approach is a higher rate of radiographic recurrence. It is thought that open surgery facilitates development of adhesions which can anchor the stomach in an intra-abdominal position. Laparoscopic repair has an estimated radiographic recurrence of about 27% at 1 year, but very rarely are these recurrences symptomatic and require re-operation.14 Some studies have suggested that the addition of a gastropexy helps reduce recurrence rates, but the evidence is mixed.14-16 A meta-analysis of laparoscopic mesh repairs demonstrated improved hernia recurrence rates compared to primary repair (12.1% vs 20.5%).17 Even when restricted to studies with at least 2 years follow-up, there was a decreased recurrence rate (11.5% vs 25.4%).17 However, not all studies were able to replicate the finding that repair with biologic mesh reduces long term recurrence. Oelschlager et al found that recurrence rates at 6 months were lower in the mesh group but there was no difference between biologic mesh repair and primary crural repair at 5 years.18 The use of mesh and the safety of its use has also been a subject of debate. An analysis of the NSQIP database found no statistically significant difference in 30-day mortality or secondary morbidity in laparoscopic repairs with and without mesh placement.19 Mesh repair should be considered when the crural muscles are too attenuated for primary repair.
FINAL PATHOLOGIC DIAGNOSIS:
A. LIVER MASS EXCISION:
Cavernous hemangioma with infarction and sclerosis. There is no evidence of malignancy.
CLINICAL HISTORY:
Paraesophageal hernia, incidentally found liver mass.
SPECIMENS SUBMITTED:
A. LIVER MASS EXCISION
GROSS DESCRIPTION:
A. Received fresh labeled "liver mass," is a 2.7 x 2.6 x 1.8 cm, firm, predominantly thinly encapsulated pink-tan tissue. The cauterized resection margin is inked blue, and the remainder of the specimen is inked black. The specimen is serially sectioned to reveal a mottled tan-white to pink-tan solid cut surface with scattered punctate areas of hemorrhage. The specimen is entirely submitted in cassettes A1–A6.
We used standard laparoscopic equipment with non-absorbable mesh available.
We have nothing to disclose.
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Citations
- Stylopoulos N, Rattner DW. The history of hiatal hernia surgery: from Bowditch to laparoscopy. Ann Surg. 2005;241(1):185-193. doi:10.1097/01.sla.0000149430.83220.7f.
- Maziak DE, Pearson FG. Massive (paraesophageal) hiatal hernia. In: Patterson GA, Cooper JD, Deslauriers J, et al, eds. Pearson's Thoracic and Esophageal Surgery. 3rd ed. Philadelphia, PA: Churchill Livingstone; 2008:233-238.
- Skinner DB, Belsey RH. Surgical management of esophageal reflux and hiatus hernia. Long-term results with 1,030 patients. J Thorac Cardiovasc Surg. 1967;53(1):33-54.
- Hill LD. Incarcerated paraesophageal hernia: a surgical emergency. Am J Surg. 1973;126(2):286-291. doi:10.1016/S0002-9610(73)80165-5.
- Augustin T, Schneider E, Alaedeen D, et al. Emergent surgery does not independently predict 30-day mortality after paraesophageal hernia repair: results from the ACS NSQIP Database. J Gastrointest Surg. 2015;19(12):2097-2104. doi:10.1007/s11605-015-2968-z.
- Ballian N, Luketich JD, Levy RM, et al. A clinical prediction rule for perioperative mortality and major morbidity after laparoscopic giant paraesophageal hernia repair. J Thorac Cardiovasc Surg. 2013;145(3):721-729. doi:10.1016/j.jtcvs.2012.12.026.
- Stylopoulos N, Gazelle GS, Rattner DW. Paraesophageal hernias: operation or observation? Ann Surg. 2002;236(4):492-501. doi:10.1097/01.SLA.0000029000.06861.17.
- Draaisma WA, Gooszen HG, Tournoij E, Broeders IAMJ. Controversies in paraesophageal hernia repair; a review of literature. Surg Endosc. 2005;19(10):1300-1308. doi:10.1007/s00464-004-2275-3.
- Nguyen NT, Christie C, Masoomi H, Matin T, Laugenour K, Hohmann S. Utilization and outcomes of laparoscopic versus open paraesophageal hernia repair. Am Surg. 2011;77(10):1353-1357. https://www.ingentaconnect.com/content/sesc/tas/2011/00000077/00000010/art00018.
- Mungo B, Molena D, Stem M, Feinberg RL, Lidor AO. Thirty-day outcomes of paraesophageal hernia repair using the NSQIP Database: should laparoscopy be the standard of care? J Am Coll Surg. 2014;219(2):229-236. doi:10.1016/j.jamcollsurg.2014.02.030.
- Fullum TM, Oyetunji TA, Ortega G, et al. Open versus laparoscopic hiatal hernia repair. JSLS. 2013;17(1):23-29. doi:10.4293/108680812X13517013316951.
- van der Westhuizen L, Dunphy KM, Knott B, Carbonell AM, Smith DE, Cobb WS. The need for fundoplication at the time of laparoscopic paraesophageal hernia repair. Am Surg. 2013;79(6):572-577. https://www.ingentaconnect.com/contentone/sesc/tas/2013/00000079/00000006/art00016.
- El Khoury R, Ramirez M, Hungness ES, Soper NJ, Patti MG. Symptom relief after laparoscopic paraesophageal hernia repair without mesh. J Gastrointest Surg. 2015;19(11):1938-1942. doi:10.1007/s11605-015-2904-2.
- Lidor AO, Steele KE, Stem M, Fleming RM, Schweitzer MA, Marohn MR. Long-term quality of life and risk factors for recurrence after laparoscopic repair of paraesophageal hernia. JAMA Surg. 2015;150(5):424-431. doi:10.1001/jamasurg.2015.25.
- Poncet G, Robert M, Roman S, Boulez JC. Laparoscopic repair of large hiatal hernia without prosthetic reinforcement: late results and relevance of anterior gastropexy. J Gastrointest Surg. 2010;14(12):1910-1916. doi:10.1007/s11605-010-1308-6.
- Ponsky J, Rosen M, Fanning A, Malm J. Anterior gastropexy may reduce the recurrence rate after laparoscopic paraesophageal hernia repair. Surg Endosc. 2003;17(7):1036-1041. doi:10.1007/s00464-002-8765-2.
- Müller-Stich BP, Kenngott HG, Gondan M, et al. Use of mesh in laparoscopic paraesophageal hernia repair: a meta-analysis and risk-benefit analysis. PloS One. 2015;10(10):e0139547. doi:10.1371/journal.pone.0139547.
- Oelschlager BK, Pellegrini CA, Hunter J, et al. Biologic prosthesis reduces recurrence after laparoscopic paraesophageal hernia repair: a multicenter, prospective, randomized trial. Ann Surg. 2006;244(4):481-490. doi:10.1097/01.sla.0000237759.42831.03.
-
Kubasiak J, Hood KC, Daly S, et al. Improved patient outcomes in paraesophageal hernia repair using a laparoscopic approach: a study of the national surgical quality improvement program data. Am Surg. 2014 Sep;80(9):884-9.
- Daly S, Kumar SS, Collings AT, et al. SAGES guidelines for the surgical treatment of hiatal hernias. Surg Endosc. 2024;38(9):4765-4775. doi:10.1007/s00464-024-11092-3.
- Kumar, S.S., Rama, M., Koeneman, S. et al. Morbidity and mortality following hiatal hernia repair in geriatric patients: a multicenter research network study. Surg Endosc 38, 3999–4005 (2024). doi:10.1007/s00464-024-10956-y.
Cite this article
Cassidy D, Rattner D. Laparoscopic paraesophageal hernia repair. J Med Insight. 2024;2024(126). doi:10.24296/jomi/126.
Procedure Outline
Table of Contents
- Pneumoperitoneum achieved via a Veress needle and subsequent placement of a supraumbilical camera port under direct visualization.
- Place Left Side Instrument Trocar
- Retract Left Lateral Segment of Liver
- Place Second/Third Trocars Completing Triangle
- Dissect Gastrohepatic Ligament
- Must always be aware of the potential for an accessory or replaced left hepatic artery within the gastrohepatic ligament.
- Dissect Hernia Sac off Left Crus
- Dissect Hernia Sac off Right Crus
- Dissect Posterior Aspect of Hernia Sac
- Identify Posterior Vagus Nerve
- Transect Short Gastric Arteries
- Dissect Hernia Sac from Greater Curvature of Stomach
- Expose Esophagus Cephalad to Sac and Identify Anterior Vagus Nerve
- Dissect the Stomach off the Inner Layer of the Hernia Sac
- Excision of Hernia Sac
- Continue Hernia Sac Dissection of Stomach
- Dissect Lesser Curvature of Stomach
- Further Mobilization of the Esophagus
- Dissect Mediastinal Pleura Tissue from Spine/Aorta
- Place Vessel Blue Loops around GE Junction
- Use the Endoloop to encircle the blue vessel loop to provide retraction of the GE junction of the stomach.
- Continue Dissection of Posterior Hernia Sac from Stomach
- Dissect Lower End of Left Crus
- Combined Extra- and Intracorporeal Knotting Technique
- Closure of the crus is done posterior to the esophagus utilizing a 0-Ethibond pledgeted suture on a straight needle.
- In an extracorporeal fashion, a half-stitch is thrown 6 times to form an “extra tight slip knot”.
- An intracorporeal knot is used to complete the square knot during crural closure.
- Ensure Esophagus Dissected and Lengthened
- Closure of hiatus in the manner shown (3 cm in abdomen) increases the length of intra-abdominal esophagus by transposing the hiatal orifice cephalad
- Align Short Gastric Arteries
- Align the short gastric arteries along the top of the fundoplication.
- Fundoplication performed with a 5.5-inch silk stitch.
- Posterior Gastropexy
Transcription
CHAPTER 1
Hi, I'm Dr. David Rattner. We're going to repair a paraesophageal hernia today, laparoscopically, in an 85-year-old woman whose main complaint is dysphasia. It's a very complex case that’s had a lot of preoperative evaluation. She definitely has an esophageal motility disorder. It has not really responded very well to the usual treatments, and she also hasn't responded to Botox injections or other things that one might do to treat achalasia or dysmotility. There's a sense among her referring physicians - and I agree with it - that there's a mechanical component to her dysphagia caused by the paraesophageal hernia. So we're going to repair this laparoscopically, and I hope that she has a good response to it. So what we’ll do is we’ll get all things set up laparoscopically, expose the hiatus - and then we'll take down the hernia sac separating the parietal peritoneum from the mediastinal pleura. Once we find out whether we can reduce her stomach without any tension, we'll trim away the hernia sac, repair the hiatus, and - in her case, I may do the most minimal of fundoplications - more of a gastropexy than a fundoplication per se. Since she's got such severe dysphagia, we really just want to straighten things out anatomically and leave it at that. If she has some reflux afterwards, we’ll treat that medically.
CHAPTER 2
Let's have a knife please. So one of the important things about doing a paraesophageal hernia - or any esophageal case where you gonna be high up - is to not put your trocar in the umba - umbilicus. Put it left of midline and cephalad to the umbilicus. Everybody's different size and shape, so it needs to be individualized. I don't think there's one formula that fits all patients. A little bit more reverse-T, please. That’s colon. That’s her colon, yeah. You know what - let’s put yours in first because you can take a grasper and push that down, and then I can get this in better. Knife to Steven. Line, obviously. Yep, right about there. Okay, let’s have a 12, please. Let’s put the next one in while you’re over there with a knife in your hands. This is where the rib is, right? She doesn't have a 12-millimeter trocar. Why don't you take this - take a bowel grasper. I'll have a knife, please. This will have to work. Should be prefect. Okay, let’s have the Alien now, please. And then the liver retractor. You lift that liver up with your grasper. There - got it. That's interesting. Yeah - don't know what that is. Looks a little like an angioma or something. I don't know what that is. It's interesting, I mean... Just drop that out of there - maybe… I don’t know what it is either, but I think we could take it out with a little harmonic scalpel. Alright, let’s fix her main problem first, and let’s do that at the end, okay? Because I think that it would be a mistake if we did that and had a problem. Yeah, exactly. Okay. Knife to Steven. Entry line here. Just below the rib? Yeah, just below the rib. You want to set up your trocars so that there's a triangle between the optical trocar and your one which the surgeon's gonna operate with his right and left hand. Let me have a grasper, please, and a Harmonic. And rotate the table towards me, please.
CHAPTER 3
And let’s - let’s see how much of this comes down first. Do you ever grab the viscous itself? Sure, absolutely, no problem - as long as you don’t put undue force or stress - it's not gonna come down easily. Okay, good. That's fine, forget it. Let's just pull this this way. Alright, Harmonic, please. We don’t even need that. We’re gonna open this gastrohepatic ligament, first. Can the table go any lower or not? Okay Steven, I want you to grab right here. That’s good there - thank you. We only have one grasper. Okay, yeah. Blunt grasper to Steven. I’ll switch when your done with this phase. If I could grab anything... So this is... Come in closer please. No. They're gonna be - the vagal branches are gonna be running up in here probably. I see. All that little white stuff there? Well, it's hard to see them, yeah, but you're right. It's probably in the that white stuff. Why don’t you switch your grasper now? Grasper, please. I’ll grab the fat up there. Come in closer with the camera. Grab it right there. That's perfect. Okay. So you always - what you do is you want to take this fold of tissue. Pull right into the - yeah. That's excellent. That's a great move there. Come in just a little bit closer still - there we go. Good. That's what we want. Incising the sac. So we'll start to incise the hernia sac here. Try to leave the muscle where god put it. So usually you can get about 270 degrees around here. Okay, why don’t you grab right here, okay? Okay, that’s outstanding. I’m just going to gently peel that off until we get a good plane going here. I’m gonna try to keep this hemostasis for as long as possible. That’s nice. That’s a good sac. There are a few muscle fibers all the way down here even. Yeah, that’s crus. Why don’t you trade? Let's trade places here, and I want you to grab this and sort of pull this down - well maybe not yet. We’re not quite there yet, Steve. Alright, that’s actually probably diaphragm there. That muscle? We'll it - it's crus that's just sort of very frayed, and it's come down onto the sac here, I think. Try to put all that back from whence it came. Let's come down through here. We want to be right underneath here. Just a smidge closer. Just pull that stuff down off of here, so we can see where we’re going here. That’s good there. Do you want to see the crus muscle, or is that just an inevitable consequence of... I'm fine with it. It’s just there - there's nothing in between. You know, she’s - there’s just nothing there, so I'm okay with this. Just get this little band right here. Oh, she's fragile. Just pull it - pull it - you know, just grab the stomach and pull that down just a little so I can get that. That's excellent. So let's pull - look down at 6 o’clock while we’re there. Let’s grab - why don’t you grab right down in here and pull on that. I would grab - I would grab - you know, that's good there because I have to just dissect even that. So maybe I... Higher up, right? I think. I just need to be able to see the margin of the crus right now without getting into the stomach, so I think this is it right here. Pleura right there. So this hernia sac. It’s gonna come into the stomach pretty shortly there, so let's look back here and stay on the muscle. Come in closer, please. The hernia sac is on the crus. Well the hernia sac is the peritoneum and pleura. Right, and that’s why when you divide it you see the muscle and the crus. Right, exactly. Because right now you’re dividing hernia sac. Yes. Yes. Peritoneum. And that's where stomach is coming in right here. Come through this right there like that. We're not hurting the stomach hopefully. Maybe it’s a short gastric coming through shortly. So this little band right here has got to go. This may be a short gastric here, so grab - if you just gently hold the stomach, rotate it towards my - towards the patient’s right. That’s good. Stop right there - doesn't have to be hard. Now, let’s stop there for a second. Let’s go over to the right side. Let’s grab the hernia sac way up in here. Grab that. Come in closer with the camera. That’s good. Let’s get that on stretch here. Good. That's excellent. Just a little bit closer if you could. Coming down here. Just gonna pull the stomach down a little bit more so we can see this better. Are we gonna choke up on this thing? Yeah, I’m gonna hand it to you. Why don’t you take this. Good - that’s good there. Okay. Here, just peel off of it. That's lesser omentum. The sac is this layer back here. Take this right down, about there. Good. Pull that over towards you and towards the feet. Let’s just look way down in this corner here and see what we can see. Now get rid of that. Those little white branches are probably vagus, right? That’s exactly right, yes. The vessel right in there, coming off. Yeah. The other crus should be right where I’m pushing - should be right through there. I'm not sure. Oh, there it is. Now that’s just experience. I didn’t see it. I just knew it - it’s about where it should be. So again, you - you just try to dissect the crura themselves - the sac themselves - and not worry about all the other structures because you - it’s sort of like addition by subtraction; once you get those things sorted out, then you can figure out where the esophagus is - vagus and all that. Let’s look right up this side here. Yep. So that should be takeable. So here. That will be back of the esophagus right there. Let’s go way up in here and see what this is. I didn’t see that same peritoneal and hernia sac because you’re inside the hernia sac. No - no, we’re not. This is - this is the peritoneal hernia sac right there. This is just mediastinal stuff, and I’m just looking for the posterior vagus, which I don’t quite see yet. I think this could be it, running right on the aorta right there and coming up. That is it in fact. Yeah, it looks like it. Yeah, that’s it right there. Interesting how it doesn’t really join the body of the esophagus. Not there it doesn’t, but this is it out here, okay? So that’s important. Okay. This is all - what we're gonna do here - that can all go out here. That’s nothing. So the next thing we’ve got to do, probably, is take down the short gastrics. Let’s stop here, Steve. Let go. And then what we have to do is take down the short gastrics, and then we have to cut the hernia sac off. Okay, so let’s grab right about here. You - you excise the whole hernia sac? I’m going to excise a lot of it. Let’s just pull this down a little bit. Stop right here. Then the nice thing is if you have a hernia this big, the short gastrics are long. They’re not short. Yeah, right. Long gastric then. If you wanna be that way, be that way. See if I care. Question is how we’re gonna get this darn, you know, crura back together. That’s gonna be the challenge. Okay, a little bit closer for me. Okay, let’s move up the greater curve now, okay? Let go of what you’re holding. Start working our way up here. Grab the stomach right here for me. Good. Just gently pull down. Tell me this is not gonna want to come down freely. I’m going to be really unhappy. It never seems to. Okay, why don’t you hold the sac right here. Usually, once you take the sac up, you’re okay. I want you to pull it out toward the left upper quadrant please. That’s good like that. Good. So now - okay. So it’s in two layers. I’m gonna peel the sac off the fundus of the stomach and find out where the GE junction is. All that stuff is gonna have to go as well, right? So what you’re dividing there with the Harmonic is... Hernia sac. Yeah. Hernia sac. Let’s get this side - this anterior side. Yeah, this is - it’s very confusing. So you don’t always dissect outside the sac? Sometimes you’re inside the sac? No, I’ve dissected out - I’ve dissected outside the sac about as much as I can, so now I’ve got to get the sac off the stomach in order to free it here. I see. Probably, the stomach is twisted in here by the sac, so you can’t like totally restore the normal anatomy until you get rid of the sac. See how this just wants to hold it back here, so grab down. Okay - actually, you know what, let’s just keep going where you are. I like where you are first. We'll do that layer first. Get in closer. So the sac actually maintains the... Exactly, exactly right. Check this first. Then we'll stop. Get a little bit of this off here. Try to get this right here. There's a little posterior vein there. That's still sac there, right? This is sac, you're correct. That's just sac with a short gastric. Exactly. Come in closer, please. So you're separating the sac from the stomach. Trying to very carefully, yeah. Yeah, I'm worried about this spot right here. I think that was all sac - I mean, I could see the Harmonic through it the whole time, but still, it's just sort of weird. Well see this, I think sac is - this is esophagus. This is - see this is clear, so that's gotta be able to go. Yeah. Are you just concerned that that was esophageal muscle? I don't know. I mean see, that's clear. Yeah, yeah, yeah. I think the esophageal muscle is actually a little higher up, but we'll just take this, keep making our way along here. Honestly, I think these are harder than the Ivor Lewises in many respects. Well yeah, I mean, there's no anatomy here. So you think you’re through the posterior sac there? That’s the posterior part of the sac. And you’re cutting into it, so mediastinum is behind you? Yes, I think so. This is where we dissected before, see? Right, that’s mediastinum. Right, so that makes this pleura or peritoneum. Yep. Just trying to get the peritoneum. Yep. The ones I’ve seen where you see a pleural, you can actually sorta see a white line, you know? Yeah, for sure. See that is the inside of this, okay? Let’s go back down here. Let’s stay where you are for a second. Pull the camera back. Let’s look down here, and let’s free up the rest of this fundus. This posterior part of the sac here. Free the fundus from the sac, yeah. So I see - I think everything... That’s crossing the crus right here should be able to go. So that’s that side of it. Now, you hold on to what you’ve got for a second because - see, if I bring this down here... So here’s the edge of the sac. There’s the anterior vagus right there. Interesting. This is gradoo. That can go. Nice. That’s actually not that bad of a PH. The one I did last week with Anna was far worse - up near the carina. Just have to be careful about the esophageal wall. Yeah. Just sneaks in on you pretty quickly. Put the scope in just a little bit farther please. Get all the gury stuff up in here. I thought you don’t need to drop the scope for this? What’s that? You find you don’t need to drop the scope for this? Most times, no. I mean, we’re all the way up here to the aortic arch. I can feel it. You can feel the arch? Well, up there. Let’s pull back for just a second, and let’s look at this again. Pull back on the scope for a minute. Okay, why don’t you grab right here? Okay, that’s good like that. Okay, good. Let me see this for a minute. Bring the scope in closer please. That’s good there. See if we can get this separated off of the esophagus here or not. Okay, so that is stomach down here, right?
CHAPTER 4
This is on the stomach, so we can definitely take this part of the sac off without hurting the vagus. So once you’ve gotten the sac out of the mediastinum, step 2 is actually to separate the stomach from the sac? Yeah, I like to because I don’t think you can accurately place your sutures without it. Yeah, because you can’t see the GE junction. Right. So why don't you regrab right here? That’s good there. Okay, good. So we can see that pretty clearly - you would agree with me. There’s not nearly enough attention to this step in textbooks. Yeah, I'm gonna draw you a diagram and say just whack the sac off, easy peasy. Well, they just say resect - resect the sac, but they don't say - or they say reduce the sac, but it’s not just reduction; it’s separation of the sac. You have to know where the - where this - you know, where the stomach stops and where the sac begins. That’s the hard part. Cuz it’s actually two - you’re outside the sac to get it off the mediastinum, and you’re inside the sac to get it off the stomach. Yeah, well usually, it splits into two layers, which is what - what I’ve done here, and I look for this areolar tissue plane to try to help me here. What do you mean it splits into two? Well see, there’s - this is sort of the anterior layer - the posterior layer we already divided. Oh yeah. So this is - this - this is vagus right here. Right here again. So that means that all the rest of this we could take. So that stuff could go. Isn’t there just one layer that goes radially around the esophagus? It seems like it’s two. It seems to me like it's often two. You have to sort of split the two layers to find - if you just stay in one, it's confusing. You can find yourself cutting right in. What you’re cutting there just seems like one layer. I know, but that's because I already took one. I think. Okay. And then the other thing is it's not uncommon to injure the anterior vagus as you go through this because you can't find it and I see it. Like you can’t even really see Belsey’s there. Yeah. So I should now be able to come underneath all this here because there's the GE Junction right where this hernia sac is attached, right? The GE junction could be right there. Yep. For sure. It’s definitely anterior - anterior vagus then, right? Because... No, it’s just becasue, see it’s attached to the sac and we’re flipping it all over the place. That's part of the issue right now. I thought anterior vagus was supposed to go into Belsey’s. Which I have in my hand. So you’ve already taken Belsey’s. See, I’m coming almost across the midline onto the lesser s - lesser curvature. Back up just a touch here. Belsey’s is usually right on top of the GE junction, but... Belsey’s is in the - right now, it's in the angle between the fundus and the esophagus on the left side, but now, see it - since I’ve taken it off, it’s in the hernia sac, and I’ve rotated it. It’s on the right side now. Yep, exactly. But usually it’s anatomically on the left. That’s correct. Like the angle of His. That’s correct. Let’s see if I can avoid that vessel, take more of this stuff off. Do patients get impaired gallbladder motility from the... What are you holding right now? I’m holding the stomach. Why don’t you grab right here? Okay, why don't you grab the sac right here, so I can see if I can take it off without getting into these vessels here. They may. There’s been studies pro and con actually. I don’t make a big deal out of it. Okay, just let go for a minute, now. Just take the stomach over this way. So you can see we pretty much cleared off the whole GE junction now. So what we’re gonna do with - so the vagus has got to be heading back into the lesser curve right? That's where the nerves of Latarjet are. Why don’t you grab right here? Right there, say. Okay, put her on stretch. Okay, and see the vagus, I think, has got to be turning. This is all stuff from the sac. Back up just a touch. So we should be able to chop all this off right over to the vagus because the vagus has got to turn back into the lesser curve, okay? So this should all be able to go. The Latarjet goes to the pylorus, right? The antrum and pylorus, yep. So it runs along the lesser curvature and lesser curvature fat. Taking a fairly generous distance away from it oughta preserve it. There’s no way it can go to here because this goes to nowhere. Yeah.
CHAPTER 5
Okay, that's the hernia sac. Okay, now - no. let's see what we got here. Go around. Twist your base. Pull on that a little bit. Can I have that harmonic back, please? So we have - we got the anterior half of the sac. We didn’t really do much with the posterior yet, which is right here. Okay, so let’s take these little stringy things and get rid of them. Come in closer. Where is sac and where isn’t sac? Where’s the posterior vagus now? I thought it was gonna be right down there somewhere. Well that looks like it right down there. Very suspicious. Very suspicious. Oh, but this is - you know what, I think it's all the way out here. See this, coming off the aorta? It's all the way out here. Jeez. So that won’t be easy to bag. Let’s see if we can free this up in here a little bit. I think it might give us… Cut through all that becuase that’s - I think this is just mediastinal schmutz, I don’t think this is anything significant. I think the hernia sac is up anterior. Yeah. The sac is up in front of us here. See, there’s the aorta right there and then the view. Okay, let’s look at this stuff here. This is always bloody back here, keep going with this. See all this stuff can go right there if I can maneuver my way in. Come on, baby. There we go. Good. Let’s just go up in here. What is this right here? Where’s her esophagus in all this? So there’s the anterior vagus right there. Here’s posterior vagus. Esophagus is right here, I believe. You can go around almost any time. Pull it back just a bit. Let’s see here what we got. Alright, come in closer. Let’s see what is this right here? Is this the posterior vagus? This is what we’re saying is posterior vagus. Yeah. Your esophagus is here. We have all this excess tissue that’s in the way. And that is not posterior vagus there? That’s posterior vagus. This is posterior vagus right there. Yeah, exactly. And we got this other gradoo with its sort of leftover hernia sac stuff here. And then we’ve got this fat on the lesser curve. Pull back just a bit. So as you can see, that’s all this stuff here. It’s very bloody. We don’t really want to deal with it if we don't have to, and then this thing right up in here is this lipoma of the GE junction - come in closer, please - which is almost always there, and it's always a pain in the ass. This thing right here. And it’s always like posterior - and it always sort of interdigitates with the esophageal muscle. Yeah. And it’s usually at like 8 o’clock on the esophagus. What is this right up in here that I’m stuck on? That may be another contribution to the posterior vagus, right? That’s what I’m thinking too. Because there’s all these anatom - I mean, I was just reading this whole... Let’s just look up in here. Keep following my grasper for a bit. I think that the main body of the esophagus is actually over on the other side of this. It's right there, so that’s the vagus. This is spine actually - not aorta, right? So I think we need to - see this purplish stuff here? I think if we divide that, we’ll get a little extra mobility. Yeah, it’s being held there. I think the aorta’s on the other side of the spine. Where is the aorta in the spine back there? This is spine right here, I think. It’s hard. Plura’s sliding back and forth across it. The aorta’s on the other side, so on the left side of the spine, right? Left side the vertebral column last time I checked. Yes? I don’t know for sure I just mean like can you actually see it pulsing in there? I can't see it pulsing here because I'm looking at it - I'm looking at things from the wrong side, but it should be down in that groove right in there. See, I think that’s all we’re gonna do here, I mean. We’re asking for trouble. Okay, let's - let's get around the esophagus here and get the blue thing in. Grab that and just lift up from that. Still got some sac back here we have to deal with. I can already see the crura. Oh yeah, I can see the crura fine. Okay, let's look on the other side here. I’m just gonna have the blue thing here. Oh, great catch. Let’s pull that down towards the femur. Let’s go there. Okay, now the loop please. Getting the fat out of the way, but I can actually try to... Yeah, why don’t you grab the back one - grab that one? Let's put them in front of the esophagus. Usually, I make the X over here. That's part of my problem. Okay, good. Got it. Okay, now pull the stomach down through the loop here and pull it towards the feet so we can get this up as high as possible. Let me see if I can get that. I’m mean, it’s close to a serosal tear. Come in closer with the camera. I don’t think so. I think you’re fine. And even if you did, we can fix it, so don’t sweat it. Alright, let’s have a tooth grasper now to Steven, please. Just grab these two. Come in closer. You’ll do much better if you're in a tight like that, yeah. So what happens if you can lift that up and over? How do things look back here? Get this extra piece of garbage to trim away - except that we don’t know where the vagus is really running through that. I think you can actually see that vagus like right there. I’m not sure that's really it because I think - see, I think it's pretty close. I think it actually isn't bowed, and it comes back in. In the hole? I think it loops. I think we got our... Yeah. This little thing. We can't really trim that. Yeah. I think we have the crura. Let's see - once we close the crura, this'll look a whole lot better. I might want to take just a little bit of this stuff down right here - not too much of it though. So is the left gastric artery pretty close by? Okay, do you have the zero Ethibonds next? Let's just look at the left crus from the left side for a minute. You can let go of that for a minute. Can I have a blunt grasper at some point? Yeah, get a blunt grasper. Let’s just look at this little area right in here. See this thing right here? This is - I wanna just get this bottom into the crus fixed. You also have to be - you have to be careful because the splenic artery sometimes gets pulled up into this. I know it doesn’t seem like it would be a problem, but it actually - I learned the hard way. That's a piece of stomach, right? Or is it? Alright, let’s come in closer so we can see better. So this little layer can go right here, safely. Agree? For sure. Good. The splenic artery is more in there while the spleen is in the chest? No, but you know what happens? Because it’s so curlycue-y, I mean it can just sort of curl up, and unexpectedly, you - you find it. The other thing is there’s a - sometimes there’s a - let’s take this. There’s - sometimes there's a, you know, phrenic artery coming off the splenic that runs right alongside that crus, and if it starts bleeding, it's just a real bugger to stop it. See, what did I tell you? See, there's a big vessel right underneath there. Could write a book of lessons I have learned the hard way. Let’s push this stuff up off the crus just so I can see the bottom of that crus and get this first stitch in correctly. This is the area I'm looking at, right there. Yeah. So you just need to sort of push up here, and that's what I want. Let's look over the top of your grasper. Okay. So that’s - there’s not much more to get, I don't think. Let’s see, if I put a stitch in there, that’s safe, right? Right. Okay. Good.
CHAPTER 6
Try the tooth grasper on that loop, and see if that gets us good exposure. These first couple core stitches will be hard. The rest will be much better. Actually, hold the two blues right now. Yeah, yes, exactly - just trying to hold it up for you. Oh okay, got it. Good, that’s excellent. Okay, let’s see what happens if you lift that up and over. Can we see? Yes. Okay, stitch to me please. The aorta right there, right? That is a true statement. Okay, let’s have the stitch. Okay, come in closer please. Back up please. Okay, you can just let that hang on the blue thing there with your - yeah, and then you can get your right hand and just snap it - cut, please. I'll tell you when. So this is a - you’ve seen this? I’m gonna make my own Endoloop basically. So it’s a half hitch, 8 times around - 6 times around. 2, 3, 4, 5, 6. Okay, now spread the two things. Snap to me, please. Put a half hitch on the bottom - everything going the same direction. So essentially it’s a granny with six throws between. Okay, now grab the tail of this, please. So that’s - or it’s a hangman's noose. Let go. Okay now expose the hiatus for me. Come in closer, please. Okay, Crystal take the light back for a sec. So it’s just like the Endoloop? Well, it’s an intracorporeal knot, but it’s not square yet. It's gonna slip unless I, you know, put some square knots on top of it, but if it's enough friction to hold that. Okay, scissors please to me. So that I can - back up on the camera. Empty needle holder, please. Come closer, please. And that's a very robust bite of the crus. That's all she's got. And the strongest part of the crura, the deepest, the prevertebral fascia, right? What did you say? The strongest part of the crura are the deeper part, the prevertebral fascia. You think you're all the way there? Pretty close, I'm pretty far down. Well I'm - you know, as much as you can get. I'm not sure that I'm - I'm certainly not on the vertebrae by any means, but... Cut this, please. Okay, so what you do is you cross them. And make a half hitch. Okay, and you hold that so this doesn't spin around and then you go six times. 2, 3, 4, 5, 6. Those are all clockwise. Spread the threads. And then one more, but it's half hitch around only one strand, okay? So you got granny on the top, granny on the bottom. And it didn't matter that you went over or under on the last one? You have to go the same direction. Everything has to spin the same way. Okay, lift up. And over. That's fine. Let's get this out of the way. And that's exactly identical to the Endoloop? The way they... Yeah, like the Endoloop, I think. I can't say it's exactly... It is. It's actually described as a Roeder's knot, R-O-E-D-E-R. A Roeder's knot. If you go look it up. German. Probably pronounced differently than that, but... Scissors, please. Some people use the term "Slipped Nissen" when talking about the Nissen down to the stomach. Right, so it looks like an hourglass, like an intussusception almost. So the problem with a slipped is just recurrent reflux, right? Well they get recurrent reflux, but they also get obstruction. It's like having a two-compartment stomach, so stuff gets stuck in the fundus, and so it constantly refluxes because the valve's incompetent above it, and they get early satiety, and they get dry heaves. They're almost like a gastric band. Exactly. Exactly. So they need to be redone. They all need to be redone. Unless they are obese. Unless they are not very symptomatic. But that's not a medically-correctable problem. And then a herniated Nissen, where the whole wrap goes up in the chest. It's very common. They may or may not be because there's actually a long series. Demister used to do Nissens transthoracically and sometimes he'd even leave them in the chest. Come in closer. And I don't think that's ideal but I think it worked. So it may not need to be redone. Correct. Only if the patient's symptomatic. It all goes by patient symptoms. Everything goes by patient symptoms. Okay, spread this out. I'll show you again. So, we're spinning this way. Which for me is clockwise, for you is counter-clockwise. And we keep spinning in that direction, and instead of going over, or on both stitches, I'm only going around the first one. Oh, that's what you mean as the same direction, right, not the same direction as your first slip knot, the same direction as your overhands. Right. Yes, yes, yes. Everything's going clockwise. Yeah, yeah, yeah, yeah, yeah. And the other thing - did you see how the hiatus is sort of triangular-shaped more than teardrop? See how big it is at the top? That's bad. Come in closer, please. It's always that way, isn't it? No, it's not. Sometimes it's more oval-teardropy, in which case it comes together much better. This is really far apart up at the top, which is bad. Why don't you use mesh? Well that's - I don't like to, but sometimes you have to. How's that for an answer? Because there's an anterior gap? Well it's just, so far the data doesn't show that the recurrence rate is lower. Especially if you've done this complicated dissection, you've got a bunch of raw surface, you hate to put... Recurrence is so high no matter what you do. Yeah, I mean, certainly I don't like putting absorbable mesh in. That doesn't do anything except cost you a lot of money. But you wouldn't put like a Prolene in? She's good and relaxed right? Okay, good. Yeah, I would, exactly. Scissors, please. You know it depends who you believe. It doesn't happen as often as you would think. Come back, please. Do you do relaxing incisions on the diaphragm? That's what I'm thinking. So that's the other way to do it is we can make a relaxing incision in the right crus, and slide it over, and then put the patch on the relaxing incision. To cover the relaxing incision. Yep. Exactly. Not to cover the hiatus, to cover the relaxing incision. No. Yes. So you don't get a para-para. That way you don't get the mesh against the esophagus. Come in closer, please. Okay. And the other thing I think is pledgets are a little bit like putting the mesh on. Because you - you don't use the mesh to bridge the gap, you put the mesh as like an onlay mesh on top of your closure. Come in closer. Oh, I see. Because that doesn't work. If you just bridge the gap, it doesn't work. It's no different from anything. Yeah, no. Alright, stitch, please. How tight do you have to close the crura? It's not covered in a lot of the books. Well there's a one-fingerbreadth... Because I've heard you want a little space. Well you want a little space, right? Because otherwise the esophagus - And the reason you want space is what? So you don't get dysphagia. You can dilate a fundoplication. You can't dilate a crural closure. I thought it was so you don't want a kink in the angle of the esophagus. Well if you look, the side, you can see, there'll be a kink. So it's not a kinking issue, it's a dysphagia issue. Yeah, pull back. Now we’re getting really close to the cava. That’s the problem with this right-sided relaxing incision up here. You’re gonna be right on the cava. So the cava is right there? Yeah, that’s the cava right there. See, that’s the edge of the cava right there. So we’re 1 cm away from it right now. I thought it’s that white thing right here. This is it - this is it up here. Yeah, that’s what I mean. And it’s right here too. Yeah, yeah - okay. When you pointed, I thought you were pointing... I pointed a little bit more inferiorly. Yeah, yeah. That’s interesting. Fascinating. No, it’s just interesting how much it like sneaks up right next to the hiatus Yeah, I know. Absolutely. You always think of it as behind the caudate, but it actually kind of comes in front of the caudate. Well the caudate is wrapped around it, right? The caudate’s like sort of like a saddle on a horse in terms of the cava. It’s just amazing how close to the top of the right crus - yeah, and there’s a phrenic vein that drains into the cava right there. Well, you can see it right there. And when you tear that... She’s got a huge phrenic vein. I know - a whole lot of hurt. I found some of these PHs have a huge phrenic vein. That’s right. I don’t know why, but you're - I’ve noticed the same thing, and it’s just a world of hurt. Snap, please. You can get into it sometimes when you take down the left lateral segments of the liver, you know, doing a foregut case open, even then it's painful to stop the bleeding. You can go a little bit too far taking down the triangular ligament, there. Dr. Rattner, how many more of these do you think you want? I think two, but I'm not 100% sure. We're down to the one at a time stage, and then see what tears. There's a one-hander for you. Now that’s starting to look - that’s starting to look respectable. Now if that’ll hold and not tear, we’re good. I'm gonna get some good light, so we can see this knot maybe. This is actually an important step. Focus right in this area here. Cut please. Cut please. Okay, snap please. This will be the last Ethibond, and then we're going to switch to silks, okay? Okay. That should be fine. Yeah. You want the silks to five-and-a-half, doctor? Yes, please - one six inch - the rest five-and-a-half. So the - the other thing that's important here is - notice how much entro - esophageal length we have now compared to when we started. We have a ton. Right - it's cuz we've really transposed the hiatus. And when we started the c - a crural closure you mean - yeah, yeah. Okay, that looks good. Nice. It looks quite good. Pleased. Blunt grasper, please. Relax for just a minute there. Let's just get things back in normal position, okay? So let's just see it for a minute. Let go of that? Just - yeah, let go of the grasper for a minute. Let's get just a panoramic shot here so we got a nice picture here of the length of the esophagus. I can see we've got all this length right there that we didn't have before, okay? So it's like two, two and half. Yeah. Something like that? It's not perfect, but it's good enough. And here's the - the vagus is up in here somewhere. And where would you say the GE junction is? I'd say the GE junction is probably right here because that's the phrenoesophageal ligament. So the hernia sac attaches right at the phrenoesophageal ligament. Where's the ligament? The ligament is like - I think it's where we cut, right there. Get a little bit of this stuff gone. The hernia sac is anchored at the phrenoesophageal and then goes cephalad to the chest. Right, exactly. And this is all hernia. That's that lipoma you were talking about. Yeah, that's the lipoma that you really - it's painful to deal with. So now you have to see if you can wrap. So I think I can just do a posterior fundoplay - I think I it's just standard Toupet and a gastropexy. It should be fine.
CHAPTER 7
So that goes to there. So if we were to take something like this. Pull that around. Okay, why don't you grab the blue thing again and pull that straight down. Go in closer. Whenever you have trouble, go in closer. Good. That's good there. Good. Okay, pull back now. Let's get this. Make sure we're orientated. So that's a - a good sign because that's a short gastric, which is what we want. We should have a line of short gastrics along this side. That's - you know you're not twisted. Pull straight down and towards - right down like that. Let's see what happens here. Especially in something that’s sort of remnant of the sac and vagus and Belsey’s left. Okay, so I think this goes like this. Let me just look at this left side a little bit more closely. There’s short gastric. There’s short gastric there. So you want to see those shape - short gastrics lined up right across the top of this fundoplication. Pull over again - down, over. It twisted a little bit, I think. I’m not crazy about that. Let's try this again. That’s the piece we really want. So we want this to be like this. Lift that up and over. Let’s look underneath here. That’s the piece I want right there. Okay, pull straight down towards the feet again. Okay, that’s what I want right there, I think. That’s pretty much what I had before, I guess. Let’s look at the left side for a just a second. Let me do this shoeshine test. Now it’s straight, see? That’s straight. Yeah. Okay, stitch please - a silk stitch please and a dolphin. This is anterior vagus right there. That needs to move this way. That’s at full thickness? Not full thickness. Look down here for a second. Is this at full thickness? No. I want a - I want a good robust bite. I want to make sure I don’t just get hernia sac. You know, that’s why you trim it off - so you know you’re - what you’re getting. You don’t want it to be full thickness. You’d like to be seromuscular to be honest with you. Okay. Come on back up to the hiatus, please. Okay, why don’t you let go of what you’re holding for a minute there? Get a blunt grasper please. This is 5.5 inches - this stitch. Really? Okay. Just hold this - hold this right at this - just - yeah, somewhere in there is fine. So I'll just grab? Yeah. Come in closer with the camera, please. Come in just a little bit closer with the camera. Come in closer. Would you say all these PHs have a component of volvulus? No. Well, by definition. But no, no, actually not, because some of what we call PHs are just type 3 hernias. They're just sort of sliding - big sliding - yeah, big sliders. Scissors, please. Another stitch, please. It's very rare. I have one... I don't mean a type two, a pure PH, I mean a 3. When it's a slider plus. Yep. Yep. Like this patent. But those, which I'll just call PH, they have... Not all. Not all. Not all. Come in closer, please. That's that fat, right? I'm just trying to keep that vagus to your side of things. Yeah. Let go for just a minute. Let's just make sure we're not twisting anything here. This is really how it wants to lie. And we can let that - I mean, the vagus - I'd like to have the vagus - so this - hold it like this. Okay, come in closer for us. I don't like the vagus to be in a stitch. Because I think when you tie the stitch, you compress the vagus. It doesn't necessarily sit in the tunnel. Yeah, you don't know whether you're compressing it or not. Let me finish that way. You know what I'm saying? Yeah. Come in closer, please. Closer still. That’s good - like that. Come a little bit closer, please. That’s not very good. Shouldn’t be an angle. Just try not to do anything bad to the cava or something like that. Cross this and this would be poor form. Okay, scissors please. Swing the stomach over towards the right. Good. Okay, so let’s... We should have that going into the liver. No. After this I need 1, 2, 3 more. Five and half - all five and a half, okay? It’s like - Sergei’s talked about the minimally-invasive mitral valve stuff. Yeah. It’s really quite impressive. It is actually. I think if I had something really wrong with me, I'd rather have heart surgery than have some sort of PCI - more definitive. Yeah, well I mean, especially for multivessel disease. It's - and it's increasingly quote, “debated,” but I think the literature is actually... Is it more and more - what’s happened with the off pump CABGs? Is that...? Off pump is ridiculous. It's going to be okay, Not that one. That one. No, that's fine. Yeah, that's fine. Just leave it. It'll be fine. Alright, so this part’s done. What we got is about 3 centimeters of esophagus in the abdomen, pedicle of sac that has the vagus nerve running over the middle of the esophagus, a Toupet fundoplication, gastropexy - twice posteriorly, twice anteriorly - and that should work. Alright, now let's take the liver retractor off, and let's figure out how we're going to do this.
CHAPTER 8
Can we have a blunt grasper, please? Stay right on the capsule of this, I think. Assume - I assume it's a benign lesion. Blunt grasper, please. Let’s me just see where is this gonna - where is the deep part or the deepest part of this is. Okay, so... It’s very strange. If I go like this, you can start coming across right next to my grasper there, right? And you can grab the white stuff right there. I’ll rotate that up for you. Hold on a sec, Steve. If I flip that up, you should be able to grab it. Okay, that’s good there. Now take the other side out. I don’t think it needs to. Let me make an incision in it. Yep, exactly. Slow speed. Keep going one more. Good. I think - almost could come at it from this angle over here. Oh, Steve, what I want to do is - it - it rotates. Yeah, see, it’ll flip like this, and then you can come right along the edge of it. Yeah. Yeah. And I think you can just come right along the edge and just chunk, chunk, chunk. Let me have the bowel grasper because I think we can hold it better that way. Hold on a second. Because I think really this needs to sit like this. Alright. Yeah, stay right on it. No, that's into it. See how you have to go through a little bit of liver. Yeah. No, you're still not doing it right. I want you to start underneath here, I'll flip it up if you want. Yes. About done. He was right. 5 minutes was a good call. Okay, good. Alright, so... Another stitch? Yeah, you - well, hold on for just a second. I think it’s coming out. No, it’s not gonna come out. So - I just wanna put a stitch in, okay? So before we do anything else, we’re gonna leave this here for just one second, okay? Right underneath here. Let's have the 0 Vicryl, please.
CHAPTER 9
I want you - here. Put your first one in just like this. Don't - don't angle too - too much, but, you know, something about like that. Okay, make sure that you’re in the actual hole of the - or cut a skin incision, okay? Good, that’s perfect. Pull back. Stay still. I was trying to... Got it. Okay, same thing on the other side. Here? Yeah - the same - what you just did - exactly the same, except you’re going on the other side of the trocar. Put the end of the stitch back in and then suture passer. Good, now we’re gonna move this like that, and you’re gonna go in just about the same hole you just went in. Okay, good. Got it. Let go. Now you’re gonna do the same thing on the other side. Okay, good. Alright, that’s that. Now, let's have the Endo Catch bag. Let me put the Endo Catch bag there. I'm going to take a grasper of some sort - anything, just any grasper. Open it up. Let's go to someplace you can actually get that to fall down to the bottom of the grasper. Yeah. Good. Okay, close it up. That looks really good there. Turn the room lights on, please. Okay, that's fine. Take that out.
CHAPTER 10
So I think that case went very smoothly. We were able to reduce the hernia without too much trouble, identified the vagi, had a nice solid repair of the crura. We’ll see whether her dysphagia improves, and we’ve removed an incidentally-discovered liver mass as well - so added bonus. Nothing out of the ordinary there. Hopefully, the gastropexy augments the effect of the crural closure, and her swelling will get better.