
Mako Robotic-Arm Assisted Total Knee Arthroplasty
Main Text
Table of Contents
Total knee arthroplasty (TKA) has been around for decades and serves as a very successful procedure to alleviate pain and restore function in a knee with advanced degenerative joint disease. Over the years, there have been many advancements in surgical technique and even more so in implant design. One of the more recent technological breakthroughs in TKA is the use of a robotic-assisted arm for enhanced preoperative planning and intraoperative guidance with dynamic joint balancing and bone preparation. This video article outlines the operative technique used by the primary author in performing a posterior stabilizing TKA in a varus deformity degenerative knee using Mako robotic assistance.
Knee osteoarthritis is a degenerative disease that causes progressive loss of articular cartilage. The incidence of symptomatic knee osteoarthritis is around 240 per 100,000 per year. Risk factors include articular trauma, an occupation requiring repetitive knee bending, muscle weakness, large body mass, female gender, increased age, genetics, race (White > Hispanic > African American), and metabolic syndrome (a syndrome consisting of central or abdominal obesity, dyslipidemia, high blood pressure, and elevated fasting glucose levels). Pathophysiologic changes to the articular cartilage include increased water content, the collagen becomes disorganized, proteoglycans become altered and eventually decrease in amount, but the chondrocyte size and number stay the same. The subchondral bone attempts to remodel, forming lytic cysts with surrounding sclerosis. Bony osteophytes also form through pathologic activation of endochondral ossification. The synovium goes through progressive inflammatory changes, eventually becoming hypervascular and increasingly thick.
The patient is a 66-year-old female who presents with a 2-year history of left knee pain without history of injury or trauma. The pain is exacerbated by prolonged ambulation, climbing stairs, and prolonged standing. Treatments tried have included bracing, anti-inflammatory oral medications, corticosteroid injections with good temporary relief, and formal physical therapy. She has a past medical history of hypertension, hyperlipidemia, and anxiety.
The patient was comfortable, well-appearing, and oriented to time, place, and person. She ambulated with an antalgic gait. Examination of her left lower extremity revealed the skin was clean and intact throughout. Thigh and leg compartments were soft. She had a normal hip range of motion without pain. Grossly, her knee was in mild varus deformity. There was a moderate knee effusion. She had a knee range of motion from 0° to 115° of flexion. She had tenderness over the medial joint line. Her knee ligament exam was stable to the anterior drawer, Lachman, posterior drawer, and the varus and valgus stress testing. Her extensor mechanism was intact, and she had no pain with straight leg raise. She was neurovascularly intact distally.
Important radiographs to take before deciding to proceed with a total knee arthroplasty (TKA) include weight-bearing AP, PA flexion, lateral, and sunrise views. Some surgeons also like to review long leg alignment radiographs. The images for this patient revealed severe degenerative changes with loss of joint space in the medial and patellofemoral compartment with bone-on-bone contact, subchondral sclerosis, and multiple periarticular osteophytes. There was mild varus mechanical alignment. The patella was tracking centrally on the sunrise view.
Additionally, a CT scan was obtained per the Mako protocol in order to perform preoperative planning and allow the Mako robot to perform accurate intraoperative guidance. The CT protocol is provided by Mako.
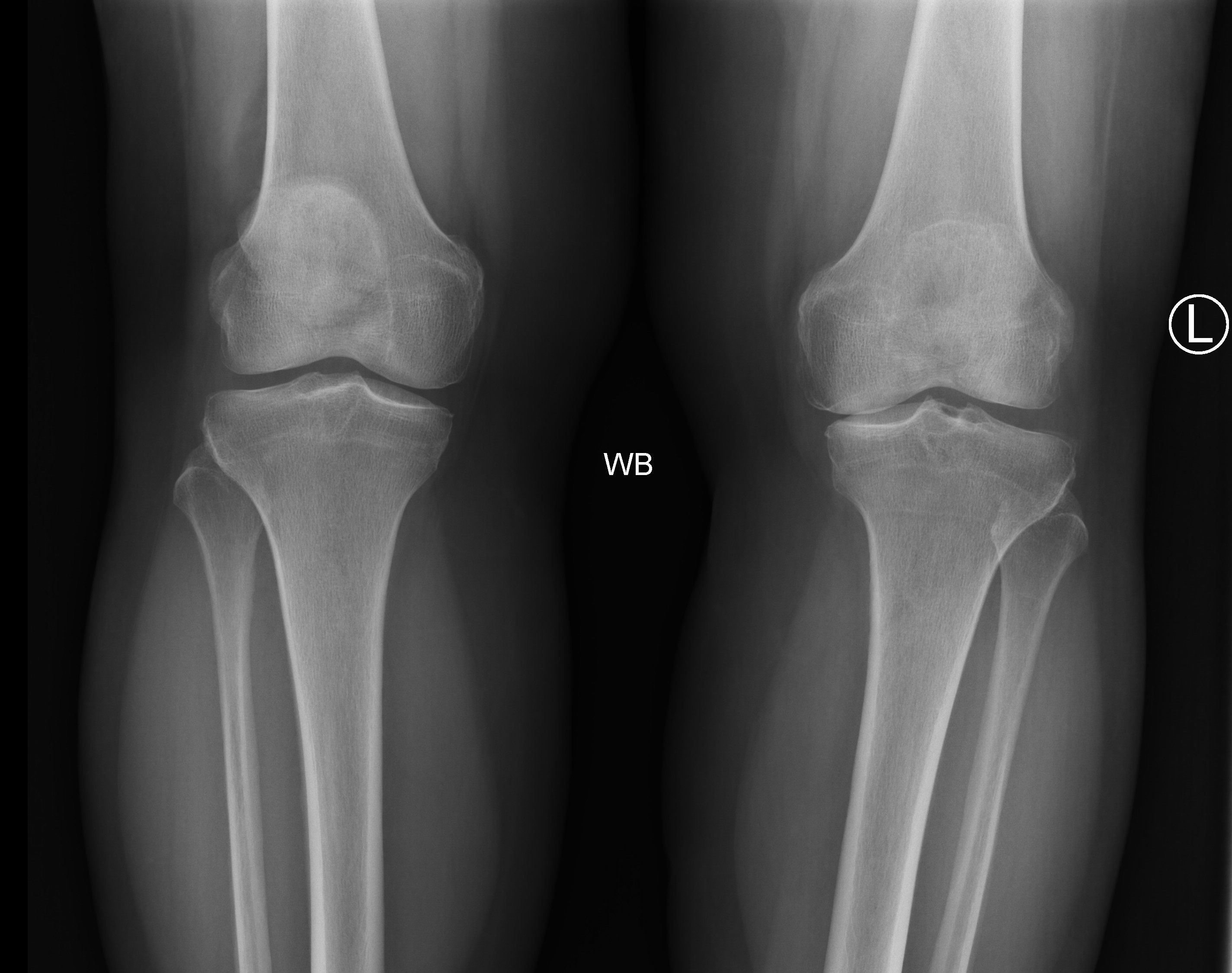
Figure 1a. Preoperative AP radiograph showing the patient’s varus deformity in her left knee.
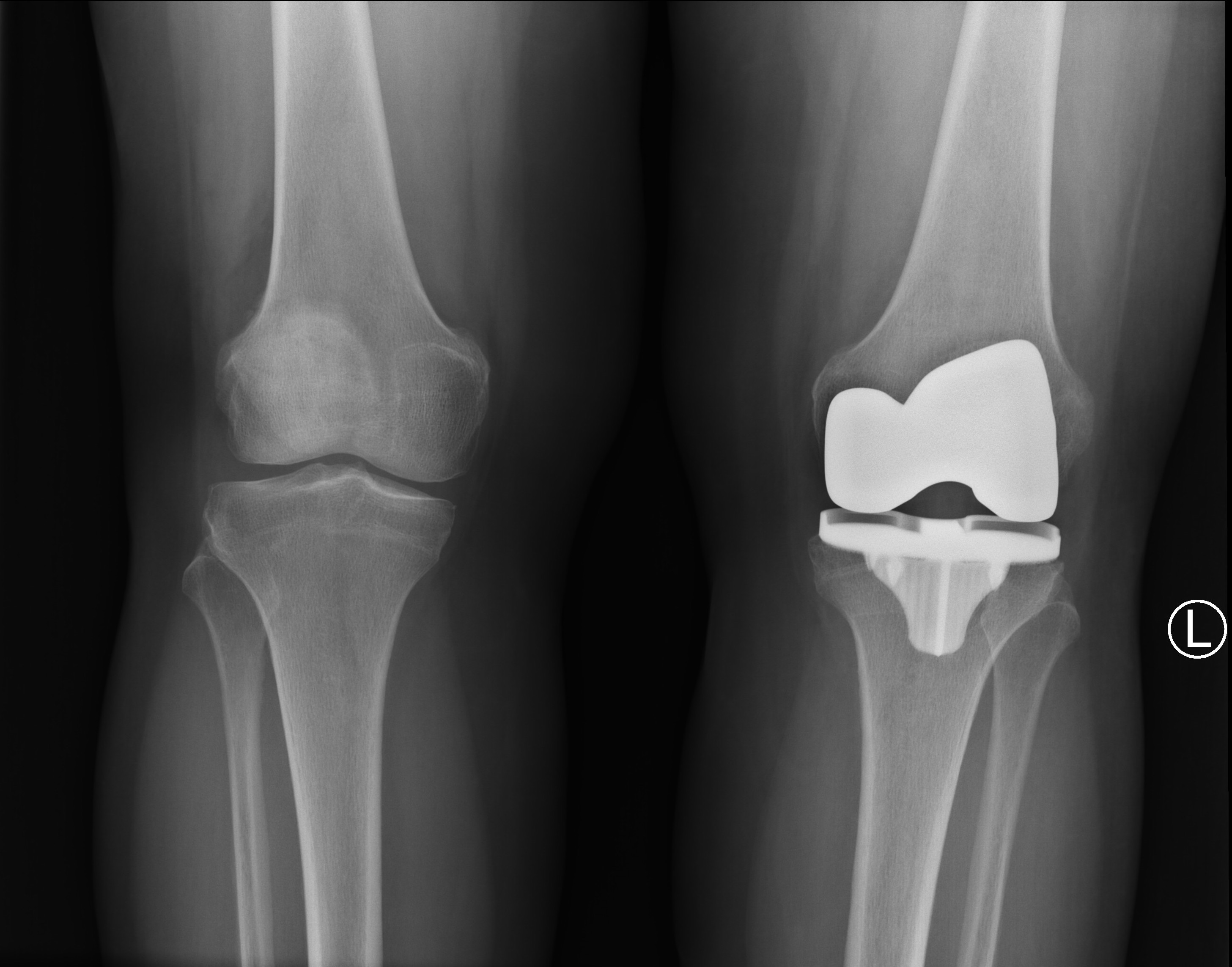
Figure 2a. Postoperative AP radiograph showing restoration of proper anatomic axis.
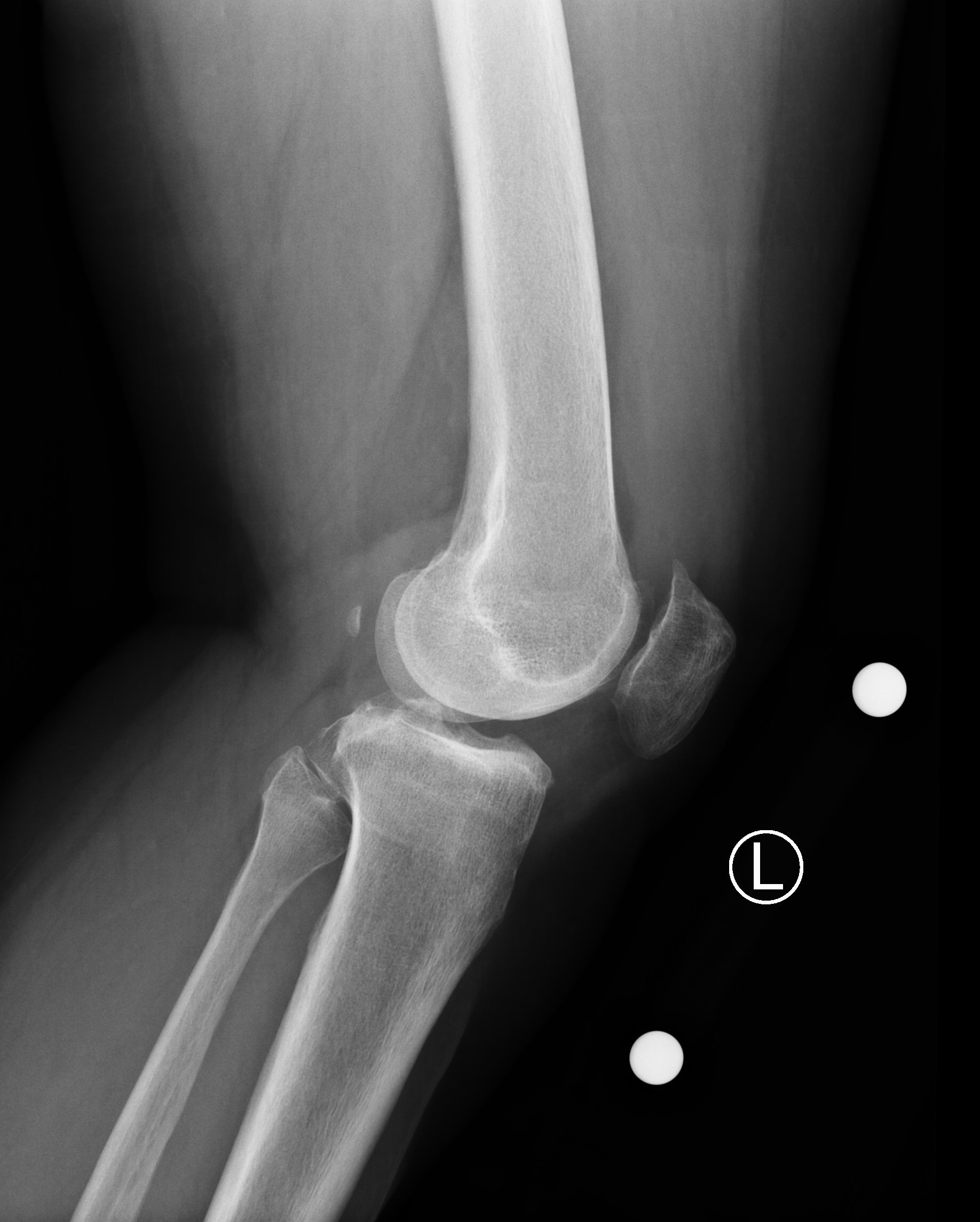
Figure 1b. Preoperative lateral radiograph showing the patient’s varus deformity in her left knee.
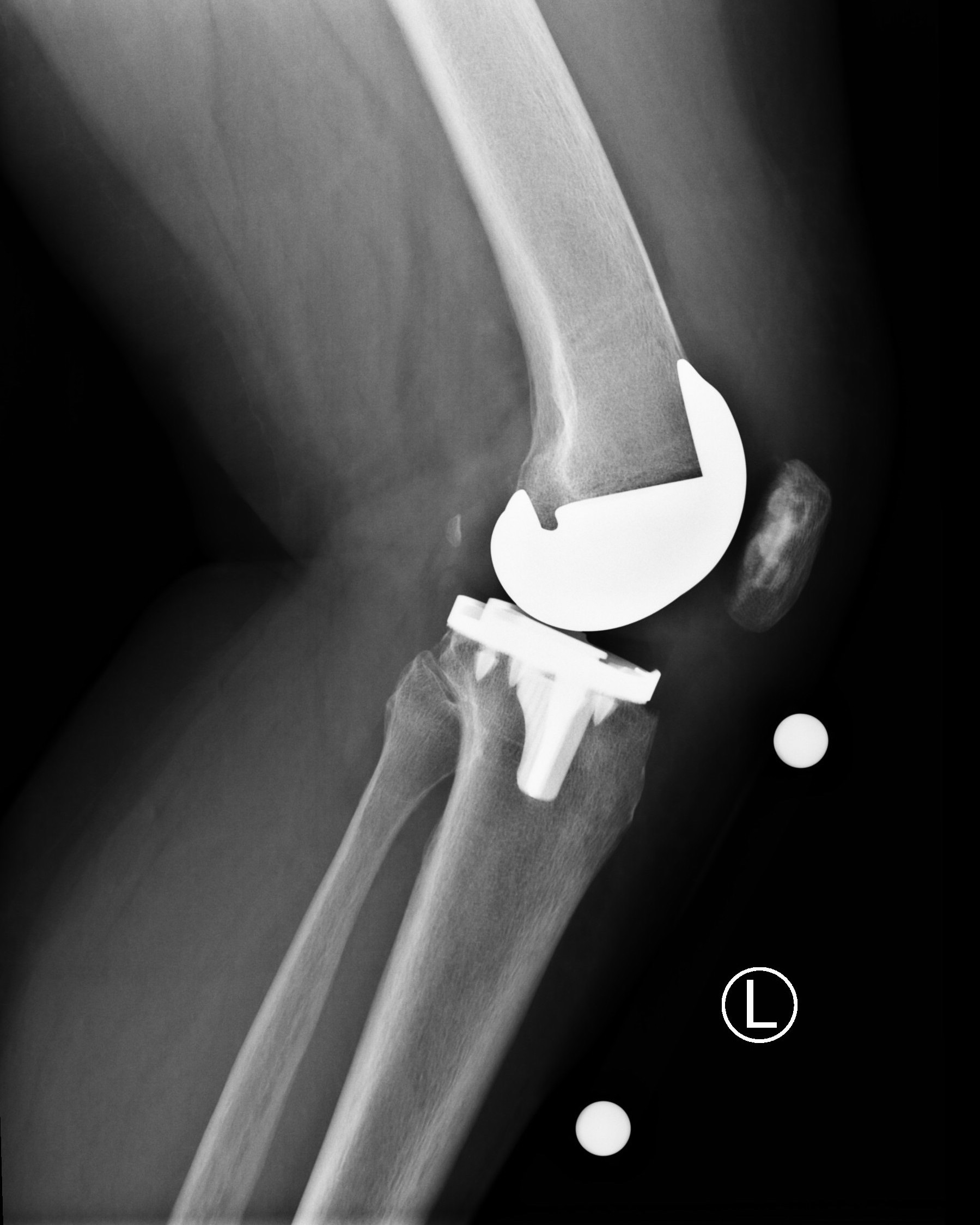
Figure 2b. Postoperative lateral radiograph showing appropriate alignment and sizing of the femoral and tibial components.
The natural history of osteoarthritis is progressive, leading to increasing pain and disability. However, the rate of symptomatic progression is variable from patient to patient. In general, it is a slow progression where symptoms become more severe, frequent, and debilitating over months to years. As the arthritis and deformity worsen over time, patients experience a decline in their function including range of motion and ability to ambulate. Some patients have severe symptoms with only mild disease visualized on radiographs while others have little to no symptoms with severe radiographic disease. Surgeons should treat the patient and his or her symptoms.
Treatment for osteoarthritic knees typically begins with non-operative management including activity modification such as reducing impact loading exercises and reducing weight. Nonsteroidal anti-inflammatory drugs (NSAIDs) are also first-line treatment. Other non-operative treatment options include acetaminophen, physical therapy, corticosteroid injections, bracing, and the use of an assistive device such as a cane or crutch. A surgical option that is typically reserved for younger patients with isolated medial or lateral compartment arthritis is an osteotomy to off-load the affected compartment and correct deformity. Joint replacement options include partial knee replacement and total knee replacement. Risks and benefits to arthroplasty are weighed on an individual basis. Risks include, but are not limited to, infection, bleeding, blood clots, damage to surrounding structures, wound healing issues, leg length discrepancy, instability, continued pain, stiffness, fracture, and need for further surgery.
TKA is a successful surgical procedure that reliably provides pain relief and improved function in patients with degenerative joint disease. The patient presented with degenerative changes of the left knee. She had severe pain associated with activity and radiographic findings of moderate to severe arthritis. She had failed to obtain adequate function or pain relief with walking aids, bracing, physical therapy, injections, and analgesic medications. Based upon these findings and following a shared decision discussion with the patient that included outlining the risks of the procedure, a decision was made to proceed with knee replacement surgery.
Patient selection for a Mako robot-assisted TKA depends largely on the judgement of the surgeon. Things to consider include sufficient articulation and range of motion of the ipsilateral hip in order to complete bone registration; the presence of metal in the operative leg, possibly creating artifacts in the CT scan that could reduce accuracy and adversely affect the operative plan; and the surgeon’s comfort level with using the Mako. At this time, only certain implants are compatible with the Mako robot, so additional factors need to be carefully considered. They include poor bone quality affecting stability of the implant; poor soft tissue integrity preventing restoration of a stable joint with the compatible implants; and the type and significance of the overall deformity in the knee, including flexion contractures and fixed varus/valgus alignment.
Osteoarthritis is the most common joint disease. An estimated 37.4% of adults over the age 60 have radiographic evidence of arthritis.1 The projected number of total knee replacements, according to the US Census Bureau, is projected to increase by 3.5 million surgeries by 2030.2
TKA, in general, has produced excellent clinical outcomes over the past few decades.3, 4 Nevertheless, there is room for improvement. Studies show mechanical axis malalignment of more than 3 degrees in up to 31.8% of conventional TKAs versus 9% of computer-assisted TKAs.5 One of the largest factors determining good clinical outcomes is proper component placement.6, 7 In one cadaveric study, the average final bone cuts and component position were 5 and 3.1 times more precise with Mako TKA when compared to conventional TKA controls.8 Therefore, robotic-assisted total knee arthroplasty (RATKA) may increase the accuracy of bone cuts and component placement.
In another cadaveric study, Mako technology for RATKA demonstrated good soft tissue protection, including no injuries to the LCL, MCL, PCL, or patella tendon. This study also demonstrated that tibial subluxation and patellar eversion were not required for proper visualization while performing bone cuts.9
Although other robotic assisted systems exist, the Stryker Mako system was used in this case presentation with a Stryker Triathlon implant. The Triathlon total knee implant has demonstrated excellent survivorship of 99% in a ten-year follow-up study.10 There have been over 2 million Triathlon knees implanted, demonstrating that it is a reliable system that is now fully compatible with the Mako robotic-assisted technology.10
The broad spectrum of disease in arthritic knees and every patient’s unique anatomy can present challenges to the surgeon in performing a TKA. RATKA technology allows the surgeon to make intraoperative decisions using a live feedback loop based on preoperative 3D CT-based templating that allows for small adjustments in bone cuts and implant placement. The robotic arm technology, including real time feedback, allows the surgeon to balance the joint based on soft tissue tension before making bone cuts. In a single-surgeon study, Marchand et al. looked at intraoperative balancing and bony resection data for over 100 knees.11 They noted that all preoperative plans were adjusted intraoperatively, regardless of the degree of arthritic disease or the type of knee deformity. The intraoperative adjustments were able to achieve balance within a 1-mm difference between medial and lateral gaps in flexion in 97% of knees and extension in 100% of knees.12 Furthermore, the majority of knees did not require soft tissue releases for balancing.12 The ability to predict joint balancing and adjust component position prior to making bone cuts results in a balanced resection technique augmented with robotic-assisted technology for precision.
Another factor in determining good clinical outcomes in TKA surgery is using proper implant sizes.13 Although not always necessary, preoperative planning can help estimate the proper implant size.14 The RATKA technology is based on a preoperative 3D CT based template that allows the surgeon to accurately predict implant size. Bhimani et al. looked at 54 consecutive patients who underwent RATKA with the Mako RATKA system that provided a preoperative implant size template. Changes in implant size were made intraoperatively based on factors such as avoidance of femoral notching, avoidance or minimization of implant overhang, and maximization of cortical contact. The study demonstrated the software predicted the exact component size of 96% of the femoral components and 89% of the tibial components, and no template was off by more than 1 size.15 Furthermore, there were no cases of notching or implant overhang on either the femoral component or tibial component.15 Other studies have shown implant size templating to be 43.6% to 68% accurate using standard radiographs, explaining the practice is not common.16, 17
As with almost all new surgical techniques, there is a learning curve with RATKA. Sodhi et al. assessed the learning curve with RATKA and found that a surgeon can become comfortable with the technology to the point of not adding any operative time within a few months.18
Some studies have reported significantly lower mean pain scores, better overall physical function scores, greater patient satisfaction and clinical outcomes, and lower Forgotten Joint Scores in RATKA patients when compared with conventional manual TKA using a variety of patient-reported outcome measures.19, 20 Although studies with longer-term outcomes and larger populations are needed with this relatively new technology, early clinical outcomes are promising.
Special equipment used in this surgery includes the Mako TKA System by Stryker.
We have nothing to disclose.
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Citations
- Dillon CF, Rasch EK, Gu Q, Hirsch R. Prevalence of knee osteoarthritis in the United States: arthritis data from the Third National Health and Nutrition Examination Survey 1991-94. J Rheumatol. 2006;33:2271-2279.
- AAOS Total Knee and Hip Replacement Projections 2030. http://www.prnewswire.com/news-releases/total-knee-and-hip-replacement-surgery- projections-show-meteoricrise-by-2030-55519727.html. Accessed 17 September 2019.
- Jauregui JJ, Cherian JJ, Pierce TP, Beaver WB, Issa K, Mont MA. Long-term survivorship and clinical outcomes following total knee arthroplasty. J Arthroplasty. 2015;30:2164-6. doi:10.1016/j.arth.2015.05.052.
- National Joint Registry (NJR) for England, Wales, Northern Ireland and the Isle of Man. 13th Annual Report. Available at: https://reports.njrcentre.org.uk/. Accessed 17 September 2019.
- Sikorski GM. Computer-Assisted Surgery and Rotational Alignment of Total Knee Arthroplasty. In Total Knee Arthroplasty 2005 (pp. 254-257). Springer, Berlin, Heidelberg.
- Hernigou P, Deschamps G. Posterior slope of the tibial implant and the outcome of unicompartmental knee arthroplasty. J Bone Joint Surg Am. 2004 Mar;86(3):506-11. doi:10.2106/00004623-200403000-00007.
- Ulrich SD, Seyler TM, Bennett D, et al. Total hip arthroplasties: what are the reasons for revision? Int Orthop. 2008;32:597-604. doi:10.1007/s00264-007-0364-3.
- Hampp EL, Chughtai M, Scholl LY, et al. Robotic-arm assisted total knee arthroplasty demonstrated greater accuracy and precision to plan compared with manual techniques. J Knee Surg. 2019;32:239-50. doi:10.1055/s-0038-1641729.
- Bukowski BR, Anderson P, Khlopas A, Chughtai M, Mont MA. Improved functional outcomes with robotic compared with manual total hip arthroplasty. Surg Technol Int. 2016;29:303-8.
- Mistry JB, Elmallah RK, Chughtai M, Oktem ME, Harwin S, Mont M. Long-term survivorship and clinical outcomes of a single radius total knee arthroplasty. Surg Technol Int. 2016;28:247-51.
- Marchand RC, Bhowmik-Stoker M, Scholl L, Rodriquez L. Balanced Resection Surgical Technique for Robotic-Arm Assisted Total Knee Arthroplasty. AOA Annual Meeting, Oct 8-12, 2017, Adelaide, Australia.
- Marchand R, Bhowmik-Stoker M, School L, Rodriquez L. Balanced resection surgical technique for robotic-assisted total knee arthroplasty. Abstract AOA Annual Meeting, Oct 8-12,2017, Adelaide, Australia.
- Gonzalez MH, Mekhail AO. The failed total knee arthroplasty: evaluation and etiology. J Am Acad Orthop Surg. 2004;12:436–46. doi:10.5435/00124635-200411000-00008.
- Hernandez-Vaquero D, Abat F, Sarasquete J, Monllau JC. Reliability of preoperative measurement with standardized templating in total knee arthroplasty. World J Orthop. 2013;4:287-90. doi:10.5312/wjo.v4.i4.287.
- Bhimani S, Bhimani R, Feher A, Malkani A. Accuracy of preoperative implant sizing using 3D preplanning software for robotic-assisted total knee arthroplasty. AAHKS 2017 Annual Meeting. 2-5 Nov 2017. Dallas, TX.
- Ettiger M, Claassen L, Paes P, Calliess T. 2D versus 3D templating in total knee arthroplasty. Knee. 2016;23:149-151. doi:10.1016/j.knee.2015.08.014.
- Trickett RW, Hodgson P, Forster MC, Robertson A. The reliability and accuracy of digital templating in total knee replacement. J Bone Joint Surg Br. 2009;9:903-6. doi:10.1302/0301-620X.91B7.21476.
- Sodhi N, Khlopas A, Piuzzi NS, et al. The learning curve associated with robotic total knee arthroplasty. J Knee Surg. 2018;31:017-21. doi:10.1055/s-0037-1608809.
- Marchand RC, Sodhi N, Khlopas A, et al. Patient satisfaction outcomes after robotic-arm assisted total knee arthroplasty: a short-term evaluation. J Knee Surg. 2017;30:849-853. doi:10.1055/s-0037-1607450.
- Clark G. Australian Experience Mako Robotic TKA. AOA Annual Meeting, Oct 8-12, 2017, Adelaide.
Cite this article
Zarin JS, Barrazueta G. Mako robotic-arm assisted total knee arthroplasty. J Med Insight. 2023;2023(214). doi:10.24296/jomi/214.
Procedure Outline
Table of Contents
- 1. Introduction
- 2. Patient Positioning
- 3. Surgical Approach
- 4. Patellar Bone Preparation
- 5. Bone Array Placement
- 6. Patellar Cementing
- 7. Robot Landmark Calibration
- 8. Osteophyte Removal
- 9. Intraoperative Ligament and Gap Balancing
- 10. Robotic Femoral Osteotomy
- 11. Tibial Robotic Osteotomy
- 12. Implant Trials and Corrections
- 13. Final Implant Placement and Check Positioning
- 14. Closure
- 15. Post-op Remarks
- Preoperative Planning
- The preoperative CT scan provides a virtual bone model that can be used to plan bone cuts as well as implant size, alignment, and position using virtual implant templates on the provided software.
- Overall limb alignment can be checked with combined femur and tibia component rotation and varus/valgus.
- Numerous fine-tune adjustments can be made on the software and later edited with more clinical and real-time information including knee kinematics and soft tissue tension intraoperatively.
- Anatomic landmarks are defined on the CT scan and a pre-op plan is developed based off that by the Mako Product Specialist who presents it to the surgeon for review.
- Preop plan includes both resection thickness of the distal femur, posterior femur, and proximal tibia and implant size, rotation/alignment, and position.
- Prep Patient before OR
- Shave skin around knee using clippers.
- Prep Patient in OR
- Patient is placed in a supine position with a safe belt over their torso and operative side close to the edge of the table.
- Typically, either a bump under the hip or a post on the lateral side of the hip/proximal thigh is used to prevent natural external rotation of the limb and keep the leg as neutral as possible. I choose to use a lateral post.
- A non-sterile tourniquet is placed high on the patient’s thigh.
- Sterilize
- The knee is sterilized using the surgical prep solution and technique of the surgeon’s choice. I pre-scrub with a chlorhexidine scrub brush, dry the limb, and then prep the leg with Chloraprep solution.
- I do not include the foot in the surgical prep, but one can choose to do so.
- Drape
- The patient is draped in the surgeon’s desired manner for a TKA.
- The drapes at the edge of the operative side of the bed should not be more than a single layer of draping over the side bar in order to place a sterile clamp on the side bar.
- Too many drapes make it too thick to place a clamp over them onto the side bar.
- Set up Leg Positioner
- There is a leg positioner provided by Mako that is attached to a sterile clamp on the operative side rail. The positioner includes a sterile carbon rail, a base which is adjustable and slides up and down the rail, and a boot to put the foot in. I choose not to use the boot and instead place the foot on the base itself.
- Set Up Robot
- The Mako robot, tower, monitor, and software are set up and positioned by the Mako Product Specialist.
- The robot comes in from the operative side and the camera is located on the opposite side. The camera needs to have a direct line of sight to the operative knee where the arrays will be placed. The robotic arm is draped and assembled by the sterile scrub technician. The Mako Product Specialist also works with the scrub technician to register the robot and its sterile tools prior to surgery.
- Conduct Surgical Timeout in the Standard Site-specific Fashion
- The Mako Product Specialist confirms the patient name, patient ID, operative side, and implant system with the surgeon.
- Either general or regional anesthesia can be used. As an adjunct, femoral or adductor canal nerve blocks can be used pre- or postoperatively. Prophylactic antibiotics are given. The leg can be exsanguinated using an Esmarch or gravity by lifting and holding the leg up for 30 seconds or more. I use gravity exsanguination and inflate the tourniquet typically to 275 mmHg.
- Midline Skin Incision
- A midline skin incision is made from the superior edge of the quadriceps tendon to the inferomedial aspect of the tibial tubercle with the knee flexed. Sharp dissection is carried down to the level of the capsule.
- Medial Arthrotomy
- A medial parapatellar arthrotomy is made. The knee is extended and the fat pad released, patella everted, and knee is flexed up again. Our patient was confirmed to have full-thickness tricompartmental end-stage degenerative joint disease that was predominant medial and patellofemoral. Osteophytes are left in place to allow for accurate bone registration with the robotic arm.
- ACL Resection
- The ACL is resected off the femoral notch and tibia insertions. I use a posterior stabilizing knee, so the PCL is also removed from the notch.
- Resurfacing
- I choose to resurface the patella in every TKA. I do this before femoral and tibial cuts. This patient’s patella measured 24-mm thick so I resected 10 mm in order to match the thickness of the patella button.
- Implant Placement
- A size 32 patella button was deemed appropriate and the lugholes are drilled at this point. Pulse irrigation is used to clean the cut surface of the patella and the real implant is cemented in place and clamped tight. The cement is allowed to harden during the remainder of the knee preparation. I cement all patella implants.
- Insert Femoral Pins for Mako
- Two 4.0-mm drill pins are fixed to the distal femoral metaphysis.
- Insert Tibial Pins
- Two 4.0-mm drill pins are fixed to the proximal tibia metaphysis.
- Place Tibial Array
- Adjust the arrays so that they are visible by the camera without any obstructions. The camera can also be adjusted by the Mako Product Specialist so that both arrays are visible throughout the knee arc of motion.
- Place Femoral Array
- Place Femoral & Tibial Checkpoints
- They should be placed in hard bone and away from future bone cuts. I place the femur checkpoint at the medial epicondyle and the tibia checkpoint in the anterior proximal diaphysis. The checkpoint locations are registered using the blunt probe.
- Hip Center
- The patient's hip is circumducted continuously and in different patterns until the progress bar reaches 100% on the software.
- Malleoli
- The blunt probe is used to identify the center of the medial malleolus and the center of the lateral malleolus. Once the tip of the probe is properly placed on each malleoli, the computer registers the points.
- Registration
- Femur and tibia registration consists of many points for each which are shown on the monitor by the software based on the CT scan. A sharp probe is used to register each point on the femur that corresponds to the virtual picture. The location does not need to exactly match the virtual picture, but should be reasonably close.
- The sharp probe is used because registration points should be collected on bone, not cartilage, so the sharp probe can penetrate any cartilage to get onto bone surface.
- It is important not to penetrate the bony surface.
- If a point is buried under an osteophyte and too difficult to access, pick a location close by on bone.
- A smaller amount of larger verification points is then shown on the monitor which need to be collected and matched up on both the femur and tibia.
- Once the femur and tibia are fully registered, I remove all osteophytes.
- Measured Resection vs Gap Balancing
- The Mako system allows you to choose between a measured resection workflow and a ligament balancing (or gap balancing) workflow.
- I use a measured-resection technique.
- Knee mechanics including knee flexion, varus/valgus, and rotation are shown on the screen and updated in real-time to correspond with the position of the knee.
- First, I bring the leg into extension and note any flexion contracture or recurvatum.
- In this case, the knee had full extension with an 8-degree varus alignment, which was lax and could be corrected past neutral to 1 degree of valgus.
- The knee was a little lax to varus and valgus throughout the arc of motion so I felt that a conservative distal femur resection was indicated.
- Software Adjustments
- Appropriate adjustments were made on the Mako software to balance and gap symmetrically.
- There are a robust number of adjustments able to be made on the software to account for the patient’s bony and soft tissue anatomy.
- The software sized the femoral and tibial components both to a size 3.
- The bone quality was good so I felt a press-fit construct was appropriate.
- The order of bone cuts can be set to the surgeon’s preference.
- The cuts are made within virtual boundaries set by the robot to protect the soft tissues.
- These boundaries can be expanded if needed.
- Dock Robot
- Distal Resection
- Posterior Chamfer Resection
- Anterior Resection
- Posterior Resection
- Anterior Chamfer Resection
- Check and Clean Resections
- Once the cuts are made, I place a laminar spreader in the joint, which allows me to visualize the posterior knee where I remove any meniscus remnants, PCL remnant, and posterior osteophytes.
- Medial Resection
- Lateral Resection
- Inject Marcaine
- In this case, the knee was trialed with a 9-mm polyethylene insert.
- The knee had a 10-degree extension lag, which I could correct with overpressure to 0 degrees.
- The knee flexed to 125 degrees with gravity.
- I felt that overall the varus/valgus stability was tight throughout the arc of motion.
- I decided to resect an additional 1 mm off the tibia.
- The robotic arm was brought back in to make the additional resection.
- The arm is able to guide a highly accurate resection, taking off exactly 1 mm more in the same mechanical alignment as the previous resection.
- The knee was then trialed again. Now, the mechanics were improved.
- The knee came to full extension and flexed to 130 degrees with gravity.
- It was stable to varus/valgus and not overly tight.
- The patella tracked centrally.
- The robotic arm is then removed from the field.
- The femoral lugholes were drilled and the box cut was made for the posterior stabilized femoral component.
- The keel punch was used at the rotation of the tibia and the 4 small lugholes were drilled.
- Tibial Base Plate Placement
- The real size #3 tibial baseplate was impacted into place.
- Femoral Component Placement
- The real size #3 PS femoral component was impacted into place.
- Both components had excellent intrinsic stability with nearly 100% bony contact.
- Liner Insertion
- The 9-mm polyethylene liner was deemed appropriate and impacted into place.
- Copious irrigation is carried out.
- The tourniquet is deflated, and hemostasis is obtained using electrocautery.
- Layered Suture Closure
- I close the arthrotomy with #2 Quill suture.
- I then use a 0 Vicryl suture to close a deep tissue layer.
- I use 2-0 Vicryl subcutaneously.
- I use 3-0 Monocryl subcuticularly.
- A sterile bandage is applied, and the patient is allowed to awaken from anesthesia.
Transcription
CHAPTER 1
Hi guys. I'm Dr. Jeffrey Zarin.We're going to be performing a Mako robotic-armassisted total knee arthroplasty today,and one of the things we'll be goingover is how we use the computer technologyto preoperatively plan for the surgery,which is one of the implant benefits related to this technique.So whenever wedo one of these operations, the –a 3D model of the patient is generatedusing the CT scan, and it generatesthe sort of three views of thefemoral and tibial bone. And we're able tomanipulate those, using the computer to havean assessment of the patient's anatomy.So in this patient, the predominant arthritis isin the medial compartment. It's a left knee,and there is a large medialosteophyte that can be seen over here –and we'll have to take that inconsideration as part of the operation.the numbers that you see on the screen representthe alignment and the boneresection relative to how we're going to plan for the surgery,and so the initialphase of the planning process is to justsize the implants appropriately to matchthe bone in a more measured resection type of technique.Then during the surgery,you'll be able to see howwe're able to use the ligament tensioning andthe kinematics in the active –or the live adjustments that can be made basedon the patient's specific anatomy related to their arthritis.So this is a – this isthe starting point, so then using the computer technology,we're able to placean implant. This uses a Triathlon Stryker system kneethat is the only current implantfor this technology and instrument. So based on this,they come in multiple sizes,but the size 3 is the one that seems to fit the boneappropriately. And this is a preliminary position,so this allows a virtual presentation ofwhere the bone resections will be.So without the implants, I get a senseof in the – in the three –coronal, sagittal, and flex knee view, I'm ableto see where the resections are going to beto allow for accurate positionof the implant. So for instance,this knee looks like it's going to takea little bit too much bone anteriorly,so you can move the target and thenflex the knee or extend the knee to adaptthe position of the implant.This would be notching the anterior femurat this amount of flexion, so –so I'll set it to where it will be. The robotic arm givesalerts for if I have too much combined flexion or extension.Right now, with the6 degrees of flexion and 3 degrees of slope,there's too much combined, soI want to back that out to about 5 degrees.And then potentially we cananteriorize the implant a little bit,and that will make for a much cleaner and closerresection to the implant. Thisis a 0-degree mechanical access that we're setting up for,but this patient hasa varus alignment that we can visualizeon the pre-op radiographs. And we'll be ableto adapt this, but I usually will take a degree of varus off ofthe tibia to undercut some of the sclerotic bone medially –and sometimes this needsto be adjusted.So finally, I check mediolateral with the implant. If wewere to go up a size on the implant, you can see how itis overhanging in the corner here, and I can check posteriorly –and it's overhanging posteriorly.So I think the size 4 is too large, so we'll downside tothe 3, which gives a much better appearance posteriorly.So there you cansee there are posteromedial osteophyteand some posterolateral osteophytethat could affect the gap and the balance of the knee.Then once preliminaryimplant position is selected, then there is a CT-based view.So focusing on the tibia here, I check and make surethat the implant is going to beright down the middle of the bone. I do usually put a few degreesof slope on the tibiadespite using a posterior stabilized construct because thissystem can tolerate that,and I feel that it matches the patient's anatomy a littlemore accurately.And the 1 degree of varus here is keeping the tibial implantright down the center of the tibial canal, so I think that'll bevery reasonable. And then the lastis checking the base plates, so looking at thebase plate, nothing is overhanging,all of the components seem to be appropriate, andit's set essentially to 0 degreesrelative to the medial border ofthe tibial tubercle.This can be adjusted during the surgery. On the femoral side, Ifirst check to make sure thatthere's not going to be an anterior notch.So the – the implant lines up very nicelyand matches the patient's native anterior bone,and medially, the contour of the single arc radius of this implantseems to match the patient very nicely.Laterally, because it is a symmetric implant,there's usually some overhangingor extended metal into the lateral side,which is very typical because of theasymmetry of the native anatomy.The last part is I check for the rotation.This allows for the placement of thetransepicondylar axis and posterior condylar axes lines,and so usually theposterior axis is 3 degrees off of internal rotationrelative to the transepicondylar axis,but in this knee, they're actually very close.And so what I try to do is mimic the trochlea, whichwould be the white side line, with the implant, so as I follow thepink line with the metal green trochlea,that's very nicely matching. So anyadjustment to that would occur during the surgeryas part of the balancing ofthe flexion gap. And last, the –looking at the AP equivalent, this looks and makes surethere's no mediolateral overhang,and as we come anteriorly, the anteriorflange is not overhanging into the lateral gutter,which it looks very closebut pretty good. So the last bit then is to make sure our resectionnumbers make sense, and so we're taking currently about8.5 mm off the distal femur, which is a little much for me.So I usually like to take between 6 and 7, so I've distalized thatto tighten the flexion gap up – and if our extension gap is tight, it'svery easy with the robotic arm to just re-plan this to be raised orlowered. Same thing goes for anterior and posterior positionof the femoral component.8 mm is a pretty reasonable medial femoral cut.It's very symmetric here. She doesn't havemuch overhanging medial femoral condylewhere – which usually there's a bigger resectionmedially than laterally.If it turns out that we're not externally rotated enough, I canpin it here, and we can externally rotate to get it to adifferent position, but obviously,that will affect our anterior resection. So I'll probably juststart with this where we had it before -maybe one more in external rotation -and then we'll make adjustments liveduring the operation based on what the gapbalancing shows. And that is pretty much the standardset up for planning the surgery.There can be adjustments during the operation, depending onwhat happens with the gaps that are done on this screen,and you'll seeduring the operationas we measure the gaps in the bottom right corner ofthe screen it will actually give objective measurementsof the extension and flexion gapmedially and laterally,and I'll be making adjustments based on the clinicalfeel of the knee as well ashow I feel it's going to release during the surgery.Once we get started,it's a standard medial parapatellar approach through a standardmidline incision.Initially when I was doing these surgeries, the array forthe robotic arm required an extra-articular pin in the tibia or in thefemoral shaft, but we've been able tomodify the position of the array so thatyou'll see the pins are entirely within themidline incision of the knee –and it's a pretty standard incision.Once the approach is complete, I prepare the patella first.The patella resection is a freehand resection for me,and I resect 10 mm,which is equivalent to the thickness of the implant, and we'llmake that decision during the operation.I do cement the patellar button in place.I think the 3-peg cemented patellar buttonshave a low complicationprofile, and so I have not been using a press-fit,but this patient hasgood bone quality and is relatively young and active,and so I have been preferringto use the press-fit implant designs without cementing themlargely because the resection bythe robotic arm is very symmetric – very consistent.And so the contact for thebone is quite good,and I have had good success with these implants. Sothe patella is resected,the cement is mixed, the lugholes are drilled, and thepatella is clamped into place.First and initially, while the cement is hardening,the rest of the knee is prepared.There are two pins placed in the femoralmetaphysis and two in the tibial metaphysisthat you will see that the arrays areaffixed to, and then the next step is to register the bone with therobotic arm and the robotic central processor.First, there is an arc of motion of thehip to create the center of the hip, and then the medial and lateralmalleoli at the ankle are registered.This will give a mechanical axis ofthe limb and can be validated with the roboticCT scan that's done preoperativelyto allow for a live intraoperative alignment assessment.Once that's done, we knowit's going to be a size 3 here, so I need to registerthe bone to the robotic armto make it match the template. So there's asmall probe that is used to touchbetween 30 and 35 points on thefemur and tibia that will register the bone to the robotic template,and that goes reasonably quickly. Once that's done,then the balancing is carried out. Sothe osteophytes will be removed subsequent to the registration,and then the gap balancewill be assessed as part of the arc of motion of the knee.So once the registration is carried out,the robotic arm is brought to the field,and then it is used to –using the haptic feedback, the robotic arm with thesaw attached to it does make the resectionswith me guiding it. There aresometimes some minor adjustments with this.Because the pins are very close in thefield, I sometimes have to position the legexternally or internally rotated to allow itto be within the field of the arm. I found that this allowsto minimize the number of timesthe base of the robotic arm needsto be moved,because when the foot is in a very rigidly fixed position, youhave to get the arm to match it – where I can move the leg.Frequently, I have to externally rotate the leg some,which isn't that big ofa deal, but the robotic arm can adapt to the position ofthe leg in space based on the arrays. And so you'll see how thatgoes when we do the surgeryto make the robotic arm accessible to the resections.It does not know where the soft tissues are, so I do have alimited number of retractors I place,but you'll see that I do not pullon the retractors or have to gainvery aggressive or extensile exposure of theknee – just enough to let thesaw blade reach where it needs to reach.Sometimes the anterolateral cornerof the tibia is hard to reach, and once in awhile, I do have tomove the robot to get that area withoutendangering the patellar tendon, but otherwisemost of the resections are usually pretty smooth.Once the resections are done, then we'llplace trial implants. I do spend some timecleaning out the posterior aspect ofthe knee, and I do a posterior stabilize constructfor the majority of my knees, sowe'll be doing some of the soft tissue preparation, and thenI'll trial the knee. Once we trial, then I'll have immediatefeedback with the robotic arm as towhere the balance is, where the alignment is, andhow we feel, and then occasionally,I'll need to make an adjustmentwith the robotic arm to reset one of the resections.Frequently, I do not, but we'll see how it goes.Once that's done, then the robotic arm's jobis complete, the preparation is done,and so the rest of the surgery isstandard for preparing the bone to accept the press-fit implants.There is a preparation phasefor drilling the lugholes and creating a box cut,and then there's a keelpunch on the tibia. Once that's done,the real implants are impacted. Their fixationwill be assessed,and then the real polyethylene will be inserted. Then it's astandard closure.All of the pins and the robotic array needs to be removed obviouslybefore the end of the surgery,and a standard bandage will be applied.
CHAPTER 2
Thank you. So this is a Stryker proprietary thing.Okay, now we'll take the big F tool.Let's see. That one looks about right.Good, and then this thing attaches.That has a sliding clamp that holds the foot.Good. Then we'll put one of these over here.Clamp to Courtney.Great, everyone over there,good, and then we'll just need your football of a bump.Good. That's our set up.
CHAPTER 3
Okay. Ready – standard midline incision.Mayo scissors.Thank you.Gelpi.And a Schnidt. Grab the Bovie, Courtney.This is all standardanterior approach. I do it in flexion because I think it helpscreate a little tension on the tissues, and so I don't have to createas big a flap – undermine as big a flapmedially and laterally – right down to theend. I'll take another Gelpi. Thank you.I'll take a sponge and a Bonney.I'll sponge these little things off.Another Bonney.Just gently raise a little medial flap here.This patient has a BMI of about 35, so we may have to create alittle bit more flap than usual.Pretty good - little bit here.Okay.
So then a standard medial arthrotomy right at the medial edge.We might need to take a little more skin. We'll see.Okay, I'll take a deep knife now, please.Thank you. Ready with the suction?Wooh – big effusion!It looked like clear fluid.I think we'll give a little more incision. Knife coming back.Can I have a Z, Ally?So she has a varus knee,which tends to be tighter medial than lateral.So I usually will anticipate by –by putting off - releasing a little more medialknee. If you can keep hermap down, it'll help me.So we'll create a little medial flap here.And we'll clear this anterior medial meniscus excision.This is all standard approach for me for a kneereplacement. I kind of remove the meniscus in stages.I take the anterior thirdhere when I can see it.Then we'll use this little osteotometo create a little space under here.A little suck in that medial corner there, Courtney – thank you.We'll just gently tease that around. Then I'll just release theselittle deep fibers of the MCL.Okay – and a deep knife. Sorry.So now in extension, I release the fat pad anteriorly.You can take that Gelpi out of there, Courtney.Yep, you can take that top one off.And that'll clear adequately.And then we'll flex this back up.There goes our exposure. And then we'll take the Z back.So I clear a small amount of the suprapatellar synovium.Looks like a 3.We'll take a deep knife, Ally.Thank you. And we'll clear this little bit of infrapatellar fat pad.Ann Marie, can you put the tourniquet up to 300?She's just a little hypertensive, and it's not holding.If your pressure comes back down, let me know, andthen I'll move the tourniquet back down.And we're just having some blow through here.Now the ACL is here.
You can see it, so unfortunately it's no useto us in a – in a total knee currently.So I'm going to resect the ACL.The patella's first, Ally, so we'll do that next.So you can see, she has tricompartmental arthritis.There's no cartilage left here. She'snot on the patella, andso – and there's a large medial osteophyte here. So –and there's a large tibial osteophyte, but as part of thisapproach, you do not want to resect those,because we need those as registration pointsfor the robotic arm – and so that's different than usual.
CHAPTER 4
So nowI'm going to do the patella next. Two triple hooks, please.Thank you.We do the patella, since this is going to be a – this will bea press-fit knee for the femur and tibia, but I – Bonney, please –I haven't quite adopted the press-fit patella technology,so I like to cement the patella still.Just resect a little of this suprapatellar synovium here.Okay.22 mm thick,so the patellas are 9 or 10 mm. I'm going tostep to my left here.Let's see the wide saw blade, please. So we'llshoot for a 12-mm thickness residual.It's still a freehand cut in my hand.Not bad – let's see how I did.Feels a little thick to me, still. Yeah, needs another millimeter.32 I bet.That feels better.Yeah, okay. You can take the pickle fork out.So here's a 32-mm patella.That looks about right to match her bone.Okay.Go ahead, Courtney – drill those.Good.Good.Let's see the button.So we were shooting for about 23 or 24 mm thick.Which that's right on 24, so that looks very nice. This...Thank you very much. Can I see the rongeur, please?We'll just clear this edge.Jess, you can show me a 32 patellar button.Great. You can open that, along with one bag of cement.Should I start mixing or...Yep, once the button's open,and you have the correct clamp ready.Also, we'll need the pins now for the robotic arm, so you have todo two things at once. Here you go, Courtney –if you can do that –the long pin on the drill and the sleeve.
CHAPTER 5
So next we're going to put in –here you go, Courtney. Next, we're going to put in the drill pinfor the robotic arm, which is one of thearray pins. Let's see the long sleeve.I've been putting these within the incision, and so it has to go –it has to go just proximal to the trochlea.You'll be able to see where it is in a second.Let's see. Let's make sure that's good.Another one.All right.And then this is one of the arrays for the femur.Do you have the blue screwdriver?So I just put this temporarily here to hold it in place, and thenwe'll flex the knee up. Suck in there, Courtney.Yep.Pretty good -–our quad tendon's okay.So we have to multitask a little bit,because we're working on pins andon cementing at the same time.Yep. Here, we'll swap this out.
Okay, now let's see the tibial pins.So these two tibial pins go intra-articularly,down here,below the tibial tubercle, and I angle them just a little bit uphill.And then the sleeve.
So this is what the array looks like for thetibia, which is – this is actually, technically, the pelvic array.And then we'll set this here.Oops – I need to angle it out a little bit.There we go. That should be all right.So I check the angle of it because the robotic array needs to beable to see these things.So this will set here. This is actually using the hip array. We don'twant it to hit her skin there, so I'm careful to make sure it'sjust close – so that looks pretty nice.Let's see the femoral array now.You can pass it to me, Courtney.
Sothis is the other one,which we'll set here.This actually looks pretty okay to me. We'll see.We get this guy to screw on there properly.So now the robotic arm gives a displayof where these things are seen by it.
All right, mallet.Okay, go ahead.Give it 2 more. There you go.That's the femoral checkpoint, and then thisis the tibial checkpoint. These –if you can't get it, I'll take it.These little things give us validated points for the –for the robotic arm throughout the case.Okay, go ahead, Courtney.Yep, keep going.Couple more – good. All right, so that's good.Let me just have that blue screwdriver,the small one, again. I just want to make sure.You don't want anything to move.
CHAPTER 6
Okay, our patella's ready.Let's see the cement, please, and do you have awet lap sponge?I use high viscosity cement for this,because it allows us to have thiscement ready quicker,and I do the cementing part of the case now becauseit will harden while we're doing the rest of the preparationand shorten the surgical time –just a little trick.Okay, we'll take the clamp. Thank you.So we'll just give it a littlepreliminary squeeze.We'll see.Take the cement off.Put the clamp back on.Make sure no skin is trapped.You have a Schnidt? Thank you.So I'm going to suck that little guy, Courtney.All right, one more right there – little one. Yep, good – okay.Here you go.
CHAPTER 7
Okay, very good. Now – now we need to set ourregistration, so I'm going to step to my left again.Okay, so first is the hip center of motion.So go ahead – no dancetoday guys. So, we sometimes do a little dance during this part,but – butthe idea is to flex and extend, internally-externally rotate,abduct, adduct, and thenit will center the head. And then we need to tell it where –that gives us the proximal point for our mechanical axis.And then thedistal point is our ankle, so that's the medial malleolus.And then the lateralmalleolus – it's a little bit subjective,but I think some of the error cancels itself out.Okay, Jess, that one's good.And then we need to tell it where thefemoral checkpoint is here for later in the case, so go ahead.Very good – and then here's the tibial checkpoint.Good, and then – so now this is the registration part of the bonefor the robotic surgery.So I've already done most of the exposure. It lookslike a lot of points, but it's actually pretty quick. So I justwant to touch the bone with this,and I'm just following the pattern closely but not exactly,because the idea isto just give this as many points in multiple dimensions.Jess, will you erasethat one? That one poked in the bone. Sorry – yeah,that's it. Thank you.So that one accidentally punctured into the bone.I felt it go through the subchondral bone,and that won't be any good for a point because the CT scan isbased on the bone itself and not the articular cartilage.So on the medialside of the knee here, where this is all the way down tothe bone, these points are great, because they will not –I don't have to worrythat I've punctured through anything ortold the robotic arm that I'm deeper thanI really am – that the bone is actually deeper than it really is inreality. So I'm just working my way here. I'm –you can tell I'm not perfectin terms of putting them exactly where the thing says to,but it's justtrying to make sure I get a broad ga –spectrum of anatomy to register – andthese are the osteophytes overhere that I did not take off, but it's crucial to removethose later because those are going to affect thegap balancing of the knee –but in the beginning you can't take those out.And then four more justover here in the notch, and then we'll see how good a job I did.There – so let's see.So we're looking for greens and yellows. That's great, sothe majority of those –those points are right where the robotic arm planned it.So that's the cartilage.It's about a millimeter thick, and if I push down, I'mright on the bone. So that one's good.So, this is a validation check.This is right on the bone, so that's good within 1/2 – 1/10 of a –couple tenths of a millimeter.That one's right on a medial osteophyte. This one'sup here in the corner right on the bone. Thisone's superior, anterior femurwithin a millimeter. You can see on the CT how it moves in thelittle box as I slide along the bone, so. And the last one's inthe notch here, which is right up on that medial wall –or on the lateral wall on the medial side,and that's it for the femur.Now we're going to bring the tibia forward a little bit,and I'll take that gr – blue probe back again.Now the same exact thing for the tibia.We're just going to hit multiple points here –and then same thing. She'sbone on bone over here medially, so this stuffis good – good for registration because it's right onthe subchondral bone of wherethe CT scan is.Then we'll come across the front here a little bit.So currently this exposureis not any more than maybe a little bit more proximallythan I wouldhave done normally to allow for that proximal couple of pins to –to hold the quad back without ripping it.And then down here.So I did not take out any osteophytes down hereeither, and we have a couple more over the front here.There's always soft bone there, so I have to be real careful toget through the tendon but not the bone –and then down by the tibial tubercle here.Do a couple going straight up.It's right through the patellar tendon, and thelast set is right here onthe medial tibia.Let's see how we did.Pretty good – all greens and yellows.Again, one red – I poked in up onthe front here, butthat still is within plenty of accuracy on the bone.So I'll be – I don't need to redo that one point.Then anteriorly, on the tibia –oops. Sorry, the probe got fell out of view. There we go.And thenI'm always careful to make sure the probe is pointing towardsthe tracking screen – oops.One of my pins is right where that one wants to be.There we go. One of those pins is right there –and then one more medially.Right there – good.That's it for our registration. It took about 3 or 4 minutes.
CHAPTER 8
Now, I can finally clear all these osteophytes out of here.So rongeur, please. Got it.So, now it's crucial to remove all these osteophytes even thoughin her knee they're not very large, so it's not a huge deal.Little bit laterally here -not too bad.And then this tibial one we have to get rid of.So we'll try to clear a little bit more of thisLet's see that 3/8 curved and a mallet.So, this is a crucial one.The MCL is right here, and the osteophyteis just under that. So, I'm going to carefully take this thing off.Clear that medial osteophyte out of there.Good - I think that looks pretty good.
CHAPTER 9
All right, so now we'll get a sense of what our knee looks like.Step to your right, Courtney,but keep your eyes on the knee if you don't mind.Okay, so this knee has about almost full extension.Sometimes they have aflexion contracture. Weactually have a little game about that, but 1 degree –it's in 4 degrees of varus – 4 or 5 degrees at neutral, and I canpush it to about 10 degrees of varus. So that – that – so she hassome lateral laxity. See that?Now medially, let's see what happens. So, I canpush her actually into some valgus, too.Do you have the little lollipops? So,there's quite a bit of translationyou can see in the knee here, whichI would call this a loose knee. And she's sitting at 16 or – goahead and catch that one, Jess, just for fun.So, our extension gap isa little loose or medial than lateral. Now, let's see the3, 4 spoon, becauseI picked this to fill in the lateral defect. So I – at rest she's 16,17 mm laterally, butI can push it to about – actually, not so much –less than I thought it wasgoing to be. So, I'm going to put one of these spoons in thereto try to jack this lateral side open.See how much – see that makes it goto 20. That's about what it felt like to me. So, now I've gota maximal spread laterally and then medially as I pull it. Kind ofhold it there, Jess. Capture that one.So, that's more accurate for her gaps.She has a little bit of a lax knee, so when I did it byhand, we were only getting 16's or 17's,but we're actually in the 19, 20 range,which is fine for me. That's a little bit loose on extension. So nowwe'll see what flexion has before I make any adjustments.So I have toset the knee to 90 degrees of flexion here.Little bit – 89, 90. Black osteotome.So same thing – it looks a lot tightermedial than lateral,and – so now we got to see what we're going tobe able to do laterally here. So, lateral gap is sitting at 20,and I can push it to 21. And medial –I can push it to about 16. Save that one.So, we're tight medial more than lateral, so to fix it – but ourgaps aren't that far off, so if we pin it right in the center,because we're going to need to externallyrotate the femur now to fix theflexion gap asymmetry.So go ahead and externally rotate it, and do one more, Jess.Do another one. There we go. Now, let's see what I can get outof this thing.So it's about – still not much change, huh?We're going to have to seewhether I get some release. Save that one, Jess.So we're sitting at – Igot a little better there, but I'm surprised by that. And I can stilljack this open, so we're still a little open –little tight medial compared tolateral. Now, I have to decide whether I want to acceptthat 2 mm difference or not.She has quite a bit of translation, I'm – so I'm alittle h – hesitant.See, I can make her get 19 medially. I'm a little hesitant todrop the medial.Let's just do it. Pin – pin the tibia laterally, and thengive it a degree more of varus on the tibia – yeah. So that shouldget him a lot closer now. We're within –yeah, we're basically even in extensionand 1 or 2 mm tighter in flexion.And now we're a little bit toobig, so – so I'vematched our extension and flexion gaps pretty good, but Ithink we want to distalize the femur 1. There – that gets her 19.And now we got to decide. Her knee is a little loose. I usuallyshoot for 18-mm gaps,but the question is – put it up one tick, Jess. I see what you'reafter there.So that – that's good because 18 is just about right for a9-mm poly, and she has a little bit of laxity in the systemhere – so I think we'll go with that.Otherwise, we'll end up needing a10 or an 11.So, that looks pretty good to me. I'm accepting that littlebit of posterolateral laxity, which is okay to me biomechanically.Some people wouldsay that's actually fine. I'd much –I'll accept that any day over medial posterior laxity.So, let's go check our resections and make sure they look okay.So, that was pretty fast. That'sa lot of adjustments relative, so what dowe have? We have –we're only taking a 6-mm distal resection medially, which isactually what I usually resect,and we're taking 8.5 posteromedial.So we're – we're creating a little bit bigger flexion gap,and we are – click on theposterior condylar access line. The – yeah. So we're –it's interesting, because our PCA is actually parallelalmost to our transepicondylaraxis on this one, which is a little unusual.Usually, that medial side is morehyperplastic than this one.It's more of a boxy, symmetric femur. So I think –we can always take more distal femur, so I'd rather be a little bittight in the extension than loose.And she did not have a flexion contracture,so I think we'll leave this – and if the knee comes out with aflexion contracture,we'll have to re-resect some distal femur, but I think we're ingood shape with this. Take the implant off for a second.Yeah, I think the resections themselves look fine.I think – I don't see any over-resection.We're taking 4 mm and 7.5 on the tibia, whichis a little bit conservative resection too,but I would rather take another millimeteroff if we're tight than add some if we're loose.And that posteromedial phyteI have not removed yet, so that'll loosen up. Okay, you can goback to the other screen.I think that'll loosen us up medially a little bit, which is good, andI don't really care about that posterolateral as much,I just feel there's some symmetrical –there's a lot of translation here and a lot of gapping. So, I don'twant to be loose, or we'll be putting a big plastic in. All right, that'sgood.
CHAPTER 10
Let's bring the robotic arm in.The cement is hard? Yes. Perfect.Okay, let's see. I need to grabthe handle here. You can let me go. That's good. So, we used tobe really anal about setting this thing up, but now I've learned tojust kind of eyeball and make sure the arm position –that's good, Jess. Stop right there.Let's just make sure I can reach the tibia. That looks prettygood, and that looks pretty good.I think we're in business. Some of it hasto do with – yeah, go ahead.Some of this we really used to be verycareful about, and they actually have – the green probe –they actually have a programto help you know exactly where this base is in space but –because I can move the foot around, I can usually get out of it.So, now we just have to validate our checkpoint hasn't moved.It hasn't. We have tovalidate the saw blade is where the robot thinks it should be,which hopefully it will mark. Sometimes this takes a second.There it is.
Okay, so nowthe robotic arm knows where the resectionis supposed to be. It looks likea relatively conservative resection, but I'm – we'renot surprised by that. And so I'mgoing to bring this close to the field. It engages, and then Ipull the trigger very gently –and the robotic arm will move to create the plane ofthe resection that we wanted.So now we're live. We're ready to roll. So –so the trigger will work.So, I move my eyes back and forth between the –the robotic arm and the screen,and that barrier that's green up there is a virtual barrier thatprotects me from going into the soft tissues.And so I'm just trying toremove the green off the end of the bone, which is the resection.Her bone is actually pretty hard,so that's where we're getting that little jitterystart-and-stop stuff.So very conservative anterior resection here.We'll see. We might have to take twomore off the distal femur,depending on how her knee balances out later,but I did that on purpose – so we'll see where we end up.Let me – just leave it right there, Jess.I just want to hit the middle one more time.So, we'll let the robotic arm realign. Good.Just want to make sure with press-fitting,we have a very, very preciseSchnidt, please – a very, very precise distal resection.
Okay, you can change to theposterior resection now.So, now will be the posterior resection. This saw bladehas a side cutting capacity too,so sometimes it gets clogged with bone in it.So – so now we're going to set for our posterior resection, so we'llget it close.Okay, the robot wants me to externally rotate a littlebit, so hang on to that. You got it, Courtney?Hopefully, that'll do it.Let's see. Yep. So that moves it into plane.Hopefully, it'll be happy.It's close, but not quite. We may need to...Okay, good.It's interesting. You have to have a soft hand with this thing,and when I muscle it a little bit,it fights me.I'm just going to flex the knee a little bit more. I think weneed a little better angle here. Let's try again.There we go.Okay, that'll do it. So,those are the posterior resections. So, we're going toswitch to the other saw blade,which is a straight ahead one. We'll take this back.The tibial tracker wasn't being seen. It was like on-and-off –on-and-off and so...Yeah, for whatever reason,it just wasn't happy with that little bit. Mallet, please –just going to clear a tiny bit of this posterior bone.Her bone quality is fine for a one of these.So, now we're switching to thestraight ahead saw blade.We're going to have to externally rotate again, I'm sure,to get that anterior resection. That looks good.That's okay. I think we're in good shape here.So, now we're going tore – put a new saw blade on the end of this thing,and then we need to revalidate the position.I think we'll be okay. I mightflex it a tiny bit more. Let's see the green probe. So, we haveto validate our femoral checkpoint here,and then we'll validate the saw position.There it is.
So, now we'll set our anterior resection. Let's see. It may ormay not be able to trigger this.Nope, we need to externally rotated the leg alittle more. You got that, Courtney? Yeah.Okay, so now we'll pull up saw – have it lined.All right, that's the anterior resection.Now we'll switch to the posterior –just stay right where you are, Courtney, if you don't mind.
I'm just going to grab the suction here.Now the posterior resection – just put a hand here.Good.If you saw the red marks before, it's not significant. It just is a halfa millimeter to a millimeter of over-resection, so.All right, that's about it – just haveto watch the patellar tendon.
The robot doesn't know where the patellar tendon is,and then last one is the anterior resection. So, let's see.That looks fine. Thankfully, my array is holding up.All right, very good – release.So – so that is it for the resections for the femur.
No cutting blocks, no pin holes –it just enacted our plan.Now some of those resections are a littlebit unusual for me because that distal resection is very minimal.And we know we're not going to notch obviously,so it made a niceanterior chamfer resection there and a nice anteriorresection itself.We don't have to put acentral bone plug in because there's no intramedullary guide.Let's see a mallet, please.Actually, we can move this back up over here.Clear that posterior bit out. Yep – you want to grab that?Awesome. And we'll grab this one,and then we'll trial a 3 femur CR.So, let's just clear a little bit of this stuff.All right, so now let's see this thing. I'm just going to make a checkand make sure all our resections are okay – mallet, please.So it has a nice fit – lines up properly all the parts. It lookslike about 100% bone contacts, so I –again, no reason to not press-fitthis thing. So I think that's fine. So I do need a rongeur.There's a little bit of cartilage herejust from a very conservative distalcut. We may have to recut the distal,which isn't the end of the world obviously. It's very easy to do.It would just be that sequence of cuts again.Okay, let's see the pickle fork.So I've learned to get – it's tempting to just move ahead and cutthe tibia next, but I have learned to clean this stuff out and gettibial exposurefirst. Do you have a rake next, Ally?Okay, put a hand on there, and we'll put a rake over here.Just suck in that corner. I want to get the rest of the medialmeniscus – Bonney, please.That was a little posteromedial meniscus here.Yep, I'm coming in front – sorry, Courtney.This is always the scary part of the case – don't want to take outthe MCL.Rongeur, please.We use this the clear the rest of this meniscus.We'll come back and get any remnant laterwhen I clear the posterior knee.Right there – and then we'll take a Z and take out the rake.So the Z will expose this medial tibial side.Yep, Smith Peterson – there's a littlemedial osteophyte, so that would release –this is going to loosen us up atiny bit more medially.Just going to clean out some of this medial stuff – oops.Okay, and bent holding. Then we'll putthis on this side – no action.Okay – very gently there – forearm and a hand – justslide over and watch the femoral array. Bonney, please.We're a little tight on the patellar tendon here,but I think we're just going to leave it.I think the quad is a little tight too.And a rongeur.Just cleaning out the meniscus.This allows easier extraction of the tibial boneonce the resection is made, I think.Doesn't have to be perfect – just get out some of this stuff.Okay, that looks pretty good.Courtney, I think we'll be all right. We have to do ourlateral rotation a little bit, but we'll see.Not too bad. Okay, so I don't have to put any major retractors infor this. We'll just bring the robotic arm and saw back to the field,and see the green probe. Sonow we have to check our tibial point,which is good, and our femoral point –I mean our saw blade, which sometimes takesa second – good, that was fine. And then we'll set this so it aligns.That looks fine. It's happy.
CHAPTER 11
So I have to be really careful not to cause any damage to thepatellar tendon with this,because the saw blade doesn't know where the tendon is,so we'll start with the medial resection.Oops, my bad – I pushed too hard.Let's try again. So I had to bring it out of the field andback in, because I pushed too hard on that sclerotic bone.So I'm just going to be careful and sneak up.So extremely sclerotic medial bone there –just had to be really careful with thatresection so I didn't jump or have anything weird happen.Now we'll work on the lateral side.
Part of it is me muscling the robot becausewe don't have enough excursionto hit that lateral side. I think I mightjust do that with the osteotome, so – because it's just a tiny bit ofanterolateral. Thank you, Courtney – that was very helpful.I don't think so becauseI can't get the angle over there enough, and her tendon isa little tight. So I just don't want to risk injuring the tendon, sowe'll just do it with an osteotome. It's just a tiny little bit in thefront that needs to crack off.\NMallet, yep.There – that's it.So now a rongeur – so that should release everything,and we'll just peel this thing forward.Yeah, it was a good decision. We mayend up with an 11 poly because of that release, but that's okayjust because I – the bone was so sclerotic medially here.I just felt we didn'thave a thick enough cut.See how thin that cut is right there?It just barely got under. It makes mewonder whether we need another degree of varus too.We should be able to dothat. Hmm – I wonder if we should do this. Jess,if you move the base of the robot, will it affect anything? Ithink we just – let me just see before we do anything –let me just look.I just need – I need more excursion this way. Can you push it ina little bit?Yeah, that helps.Yeah, that's good. Let's give that a try. Yeah, that's fine.I just want to catch that anterior bone there. There's a little lip.This is – we're improvising a little bit herebecause this lip hasn't happened, but fora press-fit, I can't leave that like that – definitely not.Now do I needto revalidate, or it's okay? Okay.All right, so we're just going to have thisthing lock itself inthere. So it'll be in the same resection plane. Thisis actually really cool.No, I think we're okay. Yeah, now I can clear it.Let's take this out.And if you could suck in the back there, Courtney, for a second.Yep.Awesome. That was really cool.We have not had to do that before, which –which was to clear that anterolateral bone. Let's see that blackosteotome again.And so the robotic arm just goes back to a perfectlocation for the resection, and there it is.Rongeur. So this is that anterolateralbone that was – you're good, Courtney –that was going to be in the way.Sorry, it's a little bloody. Our tourniquet doesn't work perfectly.All right, I think that looks pretty good.Now we'll test the tibial base plate.Yeah, size 3 looks good,so let's see a flat laminar spreader. Now we'regoing to check and see how we did. Yep, you can take that Z out.Then we'll check this gap.Oops – I'm stepping on the medial lateral meniscus there.It still looks a little tight for a 9.I'm glad we took that 2 extra. Bonney.Now the flexion gap also does loosen up somebecause I take out the PCL.I kind of wounded it before, but I never really totally cleared it out.I know some people would say this is – the robotic arm is a greatreason to do cruciate-retaining knees, becauseit really allows you to balance a kneevery precisely, and one of my main reasonsfor moving away from cruciate-retainingknees has been I I feel my own inadequacies.But that PCL looks prettygood, but I just have –just have transitioned into being a posterior stabilized person,even though I thinkretaining thecruciate ligament here would have been very reasonable.In knees that aren'tterribly pathologic like this one,I usually leave the PCL until this part,I don't think it does much. It loosens the gap up a little bit,but knees that are very pathologic,where the PCL may be very tight or very incompetent,I will take it out in the beginning before we dothe balancing.But I don't think it's going to make much difference in thisknee, so I just decided to take it out now.And a little bit of the anterolateral horn – or the posterior horn inthe lateral meniscus, and then a little posteromedial meniscus.I spend more time thanI used to even in the back of the knee just making sureeverything is nice and clean and cleared. I thinka lot of unhappiness fromknee replacements comes fromimperfect job back here, so a little bit of –obviously protecting the PCL.Do you have the Stryker curved osteotome?We know there's a posterior osteophyte here,so I'm going to go after it with this.The gap's looking pretty symmetric. It looks like a 9 still,so I'm just going to clear this posterior osteophyte hereand medial osteophyte.And the grabber.So that's the majority of the posterior osteophyte.Let's just feel – pretty good. Itry to guess what the implantsize will be to make sure we resectenough and it doesn't impinge. Little bit more lat –medially here. Let's see that osteotome again.There we go. Let's see that grabber.May need an angled curette if I can't get this.Oh no, I got it.There, that was theposteromedial osteophyte we saw on the scan. Yeah, thatlooks good.Now we'll flip the other way, so a nice symmetric looking gap. Itlooks about 9. We'llget an objective measurement in a second here, but I'mjust cleaning out the back of the knee. Maybe we can adjust thislight a little bit. Pardon my reach.There we go – Bonney again.So now there's a little remnant of the lateral meniscus here.I always feel like the progress of the case comesto a screeching halt atthis part because we got to really spend timeand clear the back of the knee nicely.Get this right over the lateral tibial edge.We'll flex it a little more. Therewe go. Let's get that osteotome now – and a mallet.So not much lateral stuff to getbecause she doesn't have much pathology here –really just trying to sculpt off any residual articular cartilage.That's good, and let's see that grabber.All right, that should do it. Let me just feel.Yeah, that feels nice and clean.Okay, we'll take the injection now.
We doa little quarter percent Marcaine with epinephrine –put a little bit in the back of the knee –little bit center. I don't put much posterolaterally.And then we make surewe get a nice subcut – subperiosteal bubble here –make sure we really get it downthe MCL sheath nicely.That's a good one. Then we'll check laterally.Nice good subperiosteal bubble there –then a little bit in the pes bursa –a little bit up in the subcutaneous anterior.Okay, now we'll find out how we did.All right, Courtney, if you don't mind stepping to your right.
CHAPTER 12
No, we can leave it – maybe in a second. Let me trial it.So let's see a 9 on the 3 CR.We're going to trial cruciate-retainingimplants because if I need to make an adjustmentI'm not committed to anything,and then the 3 CR femurmaybe an 11. We'll see what happens here.All right.All right, now we'll see how we did with our balancing whether Iget punished by taking that extra millimeter.No, I think it's going to be good.So we'll scoot that over, so now let's see what we got. So westill have a little bit of a flexion contracture,which we thought might be a concern,and in flexion, our gaps look very nice – 19, 19 – so – and there isno instability. If anything,we're a little tight in both directions, Jess. Not sure I – clinically,it doesn't look like a flexion contracture to me.I don't know. That –I would say that's a flexion contracture, so I thinkshe's pretty straight even though that thing is saying 6.I said I would never accept that,but let's see.It's a very firm, rigid knee, you know? If we take one more offthe tibia, it will loosen us up globally, which I think may not bea bad idea. The tourniquet is still up – so that will – that – that's –my patellar tracking is not perfect because of the quad.No, because I think thepatella is going to track fine.It's just a question of – a judgment callnow whether I think this is done,or we need another millimeter off the tibia.The MCL feels fine.The overall balance has very little varus, valgus laxity throughoutthe whole thing. I would say it's a little on the tight side. Let'sdo one more off the tibia, and – and then that will just take asecond. Let me see the handle to pull the femur.So we're going tomake an adjustment to – I think the knee is a little tight kind ofall the way around, and so we're going to –we're going to take another millimeter,which puts us up to what? 8.5 lateral?Oh, you did it already?Okay.Yeah, pickle fork.Yeah.I would go ahead and drop it. It's okay.I'm not convinced that's what it took.All right, bent.Just being extra careful here to add a little bit of a –gap. I think that's going to be fine – and a Z.Okay, I think you're good, Courtney.All right, we'll bring this back in.Let's see our green probe one last time.So that's good, and we'll check the saw blade.So literally, we're making acorrection by 1 millimeter here,which is an unusual thing. I have not recut much.There we go. That – maybe I wasn't in the hole.There it is. Okay.All right.Let me see the Schnidt.Yep. All right, so one more resection.This, ironically, is the real power of thesaw blade in that it can do this. All right we'll do the medialside first,because that's where the bone's really hard.Much better – we're under the subchondral bone now.I like that cut a lotbetter actually. I'm glad we did it.All right, sorry for the mess. Okay.Yeah, thanks Courtney. Suck all that in.This is a little lip upfront. Yeah, rongeur.Just put a hand there for me,and then we'll trial it again and see where we are.Yeah, actually that's all fine.That's all fine. Okay, let's trial that again.Let's take these out and see.That cut looks better.It was right through that subchondral. Maybe therewas a little bit of bone marrow or somethingthat was making it tight.Okay – and the femur.All right, mallet.All right, that's pretty good.Yeah, that feels better.Yes. Everything about that's better. See, now we've got ourflexion down to 3° only, which is much better.The mechanical alignment is 2° and20s, which is fine, and there is now a little bit ofplay, which is much better too.The patella I'm not worried about becausethe tourniquet is still up. Yep, everything about that is better. That1-mm difference makesit a much happier knee. So we'll mark our femoral rotation –tibial rotation, I mean, relative tothe femur. Okay, and we'll flex this up.Okay, you can deflate the tourniquet now.And we're good with the robot.I'll take the femoral lug drill next, please.So now that's it for the robotic part of the case.We've accepted everything.Now I just got to finish the bone preparation to put the implants in.Let's make sure all the positions look very good,so we'll drill the lugholes.Okay, femur remover – the black handle – and the tibial handle.So now I have to take the arrays off because these pins are in the way.I may need a Schnidt.These pins are in the way of thetibial base plate,so we'll take that out. I'll take the rongeur. Yep.Keep pushing toward the patient.Perfect – grab the other one.Here comes the femoral checkpoint. We got to get allthese little sharp things out of here.Tibial checkpoint – all right good. There it is. Yep, pull those twoguys. Drop your hand a little bit. There you go.Perfect – one more. Then we'll take the whale tail. Got it.Perfect. Okay, so now...Okay. Let's see the cut – box cutter.So this is standard issue now. We're back tomaking the resection for the box cut – and a pin on thecall-it adapter.Perfect. Then we'll use a long-headed pin. Courtney has it.Right in there.We'll take – that's fine, and we'll take the recip saw.Thank you.I know it's sad to take all this good bone out of here.All right, I think that looks pretty good. Here you go.We'll trial the PS - thank you.We'll just make sure this fits the way we like.That looks pretty good to me.There's a little soft tissue caught, but that'll be all right.We'll take a lap sponge.Pickle fork.Awesome.You're doing great Ally, thank you.
CHAPTER 13
Next, we'll punch the tibia with the press-fit stuff.All right, Courtney, you got that? Yep.I'm going to switch the bump up to the front.I think it was a good call to take that extra millimeter.She was justa little tight. Forearm and a hand –great. I'm going to just move this light.Okay, good.Now we'll take a Schnidt with the number 3 tibial base plate,and then two little headed pins.So, I marked the rotation when theknee was in extension.Make sure this is sitting nice and flat, because itwas a recut. Oh there's soft tissue – that's why.Yep.There we go.Yes, just the 1 to 3 one.Okay, little headed pin – so I set the rotation in position.Another one of these –that's the hardest part of the case – handing that off.All right, that looks pretty good, actually.You can open up the size 3 tibial base plate, please.That looks good. Now we'll take the tower punch.Yep, and the little punch, the press-fit one.That's correct.\N3?Correct.So this just creates the keel.Her bone quality is good, so I think press-fit is a good choicefor her. Sorry for the mess.That looks nice.And then we'll take this guy out.Maybe. Here's your two little pins back, and then this thingcreates the space for the four little lugholes. Got to make sureit's nice and flush. That looks good. And then a little sharp drillprepares for the lugs. One, two, three,four. Okay. I'll take a Kocher or a Schnidt – maybea Schnidt is okay.Good – and then the real tibial base plate.So since it's press-fit,we don't have to do any cementing. I just haveto make sure everything is clean.Good. We'll use this little lap sponge here.All right, let's see.So this is the real base plate. It has a titanium – it's a titaniumbase plate with aporous coating and four little spikes here. So the trickto this is it's got to go straight down. She does have that littlecyst, huh?Sorry, I just saw a little cyst here. Oh yeah, it's nothing. It's okay.We'll just set that carefully in there.Give it a little pull. Okay, mallet, please.So –so we'll just get this started,and then we'll make sure there's no soft tissue anywhere.That looks okay.That looks okay. I need to bring my hand forward a little bit.It looks pretty good.All right, now we'll just do a check and make sure there's nosoft tissue anywhere.That looks fine.I think we're right on the lateral edge there. Okay, double banger.Let's see that Smith Peterson.I just have a little bit of – actually I think it's soft tissue.Yeah, it's all mostly soft tissue there –make sure there's not any debris.That looks good.Check the lateral side. Yep,we're right on the edge. Okay, up and over.
Okay, you can open the left 3 femur PS press-fit.Go ahead, Courtney.We'll take the 9-mm CR trial.The tourniquet is down, so now it's always a little bloody.We'll take the CR trial, please - 9 for a 3.The CR one, please.We'll do that one next, in a second.There – and then the femur.So this is also a press-fit coated component thathas beads and hydroxyapatite on it.All right, mallet, please.Same thing –we just got to make sure nothing is stuck and that it's straight,because sometimes these can be a little tight.So far, so good. Yeah, looks pretty even.Good.I just check. Let's see the double banger. My side needs to godown a millimeter.Okay, yeah – just needs to angle toward me a little.I got it now.Good – nice secure fit.So, yep – we'll just check with the CR one more time.Looks good. Tourniquet's down,so the patella is tracking perfectly again now. So thatlooks very good.
Now we'll just do one last check posteriorly,and we'll check the real polyethylene to make surethe mechanics don't change any even thoughI don't think they will.And we'll just check lateral. Do you actually havethat straight Hohmann?Thanks, let's just look in the back –make sure there's no osteophyte or anything funny back there.Do you have a little bulb squirt? Well,anything? No, that's soft tissue. There's no cement, so.That looks fine.Let's check medially.Suck back there Courtney– yep.Yeah, the osteophyte's fine. It's not over-hanging.And then we'll check laterally –the systematic checks.Oops – there's a little something there – Smith Peterson.There's always a little lateral osteophyte.The rest of that all looks clear,and then we'll check medially with a Schnidt. Got it.That all looks pretty good. And let's see this one. This is the realpolyethylene PS trial. Let's set it in.Nice – got a little soft tissue trapped in here.Good, so nice straight knee – not hyperextended,no flexion contracture, stable as can be,really no varus / valgus laxity – but it's better than it was. It has atiny bit of toggle, which is good. The patella tracks perfectly.The flexion to gravity istons – 125 probably,and I can over-push 140 probably – but she won't getthat. She'll probably get about there.Very nice. We'll take the 9 PS for a 3 – X 3 – thank you. We'll take it.Okay, very good. We'll take the real poly now.Here's the real polyethylene. Posterior is stabilized –no soft tissue.There, that's good – and a Schnidt.There's always a little fat pad that wants to get stuck in here.That's pretty good. I'll bring it forward.Make sure nothing over there – that's good.Yeah, that's good. Got that right like that, Courtney?All right, we'll give it a little love tap.Yep, try and stay on the poly. That's it!It's good. I think I came out nicely.What's that?Okay, do we have a clean – clean stuff to put down here?
CHAPTER 14
Do you have a clean lap?Thank you.All right, two Kocher's –and the quill.I set the tension of the extensor mechanism here.That's why the attending move is the Kocher's.Put it right next to it – perfect.I'll take a number 1 Vicryl.We'll put a stitch in the fat pad.I thought this knee might be likeslam dunk for balancing, and I'm gladit had to make a couple of adjustments\Nso we can show how we do that.I run a 0 layer in the proximal adipose tissue here.We made two good decisions, which wasmoving the robotic base to get the anglebecause the lateral part was hard, and then the 1 mm.It's amazing what a difference, but it went from6-degree flexion contracture to 3.\N3, yeah –For that 1 mm.I think that sclerotic bone may\Nhave deflected the saw up a little bit.Maybe.And then when we went under it, it was – it actually tookmore than a millimeter of relative bonebecause that sclerotic bone...\NIs left over, yeah.All right guys, thank you.
CHAPTER 15
The surgery is complete. I think everything wentvery smoothly.We did have to make a few adjustments, as I had spokenabout before related to the implants. You –actually, I'm pleased that some ofthat stuff happened because most casesI do not need to make any sort ofrecuts or robotic position changes,but I felt the knee with somewhat tightwith the gaps relative to where the gapswere being predicted bythe robotic arm –and so I decided to resect the tibia some more. I think therewas some very thick sclerotic bone medially,and so that may have deflected thesaw blade a little bit – and that madethe gap a little tighter than planned.But once the re-resection was done, Ifelt the knee balanced out very nicely.The mechanical axis was reconstituted appropriately to 2 degrees, whichis what we had planned.The patella was tracking very nicely, and all of the implantfixation was excellent.You can see how there were adjustments that were made, andthe large learning curve for me with theserobotic surgeries has largely been knowinghow to adjust and balance a kneewith the capacity that we haven't donebefore. There was some very quickset adjustments I made to externally rotate the femurand bring it anterior a little bit, which loosened our gap in onedirection and tightened it in another.And then I did accept a little bitof imbalance in the posterolateral corner,which is a normal biomechanical laxity for apatient that does not have muchdegenerative change posterolaterally, and it turned outthat actually balanced out very nicelyonce the real implants were in place. I think the medialrelease as the surgery was carried throughdid release the po –the joint space medially enough to create a symmetric gap.And overall the arc and stability was excellent,so I think the surgery went well.I think the overall timing is very similar to the amount of surgery. Itwas about a one-hour tourniquet timeeven with the two adjustments – even though I dodeflate the tourniquet before the implants are put in forpress-fit implants.I think overall everything went very smoothly.You can see the potential forthis technology as we get better at understandinghow to balance these gaps and usethe power of the technologyto make very fine-tuned adjustmentsbefore and after the surgery –really I think has the potential to bring in outliers,improve the mechanics in terms of a kinematic approach,understanding and appreciating the mechanicalaspects of it can marry those two things togetherwith this technologyin a way we've never really been able to do before by freehand.