
Bilateral Posterior Retroperitoneoscopic Adrenalectomy with Cortical Sparing on Right Side
Main Text
Table of Contents
Cortical-sparing adrenalectomy allows for resection of adrenal tumor(s) while preserving unaffected adrenal tissue to prevent adrenal insufficiency. This is especially important in patients affected with bilateral adrenal tumors, typically pheochromocytomas.
Posterior retroperitoneoscopic adrenalectomy (PRA) allows for a minimally invasive approach to adrenal gland resection compared with the more traditional laparoscopic transabdominal adrenalectomy and open approaches. The PRA technique is increasingly used by high-volume endocrine surgeons throughout the world. This approach is ideal to address patients with bilateral disease and was used in this case of a patient presenting with bilateral pheochromocytomas in the setting of multiple endocrine neoplasia 2A syndrome.
Posterior retroperitoneoscopic adrenalectomy (PRA) was first popularized in Germany by Walz and colleagues. The adrenal glands are accessed via a retroperitoneal approach using laparoscopic instrumentation and CO2 insufflation.1 In doing so, the surgeon avoids entry into the peritoneal cavity and mobilization of surrounding viscera, including bowel, liver, spleen, and pancreas. Compared with open and laparoscopic transabdominal adrenalectomy (LTA) approaches, this technique promotes patient recovery with decreased length of stay, less pain, and reduced risk of ileus.2-4
One of the advantages of PRA is that it enables bilateral access to both adrenal glands via a minimally invasive approach without requiring patient repositioning during the operations.2 Patients presenting with bilateral adrenal tumors, typically pheochromocytomas due to Von Hippel Lindau (VHL) or multiple endocrine neoplasia type 2 (MEN2) syndrome, are ideal candidates for this approach. In both disease processes, bilateral tumors frequently occur. As such, patients may require bilateral adrenalectomies to achieve a biochemical cure.
In order to prevent postoperative acute adrenal failure (Addisonian crisis), cortical-sparing adrenalectomy can be performed. During this procedure, the culprit tumor tissue is removed while preserving normal adrenal tissue.5 Traditionally, this technique has been described alongside open and LTA approaches; however, for bilateral disease, the PRA approach is increasingly being utilized with success.
The patient is a 31-year-old female who presented with biochemically unequivocal bilateral pheochromocytomas. She had symptoms of hypertension and palpitations, which prompted further investigation by her primary care doctor. Her laboratory workup was significant for elevated free plasma metanephrines at 642 pg/ml (reference range < 57 pg/mL) and normetanephrine at 2284 pg/ml (reference < 148 pg/ml) as well as elevated urinary metanephrines, consistent with a pheochromocytoma. Cross-sectional imaging included a CT of the abdomen with IV contrast. The CT revealed bilateral adrenal nodules with precontrast Hounsfield units and overall imaging characteristics of bilateral pheochromocytoma (Figure 1). A close review of her imaging demonstrated normal-appearing adrenal cortex tissue on the right side (Figure 2) that would be conducive to cortical-sparing adrenalectomy on this side.
Because of her young age and the presence of bilateral tumors, she was investigated further for other MEN2A-associated tumors, specifically medullary thyroid cancer and primary hyperparathyroidism. She was indeed found to have an elevated serum calcitonin level of 229 pg/ml (reference < 5 pg/ml), and ultrasound and fine-needle aspiration findings were consistent with medullary thyroid carcinoma of the right thyroid lobe. Her serum intact parathyroid hormone and calcium levels were unremarkable.
CT and MRI are the primary radiologic techniques used for imaging normal and abnormal adrenal glands. On CT, pheochromocytomas are often well defined from the surrounding tissues and typically demonstrate precontrast Hounsfield units of 30–40. Smaller lesions tend to appear simple and solid, while larger lesions may have more cystic characteristics as well as other complex features. On MRI, pheochromocytomas have a classic “light-bulb” appearance on T2 weighted images. Functional imaging may also be obtained, especially when metastatic disease is a concern. The most common method is use of 131 I- and 123 I-metaiodobenzylguanidine (MIBG), which is an analogue of norepinephrine and localizes preferentially to sympathomedullary tissues.6
We prefer the patient to undergo either adrenal protocol CT or MRI within approximately 3–6 months of the operation for operative planning. In this case, the patient was referred to us after having a CT showing bilateral adrenal masses with imaging characteristics suspicious for pheochromocytoma. In a detailed review or her imaging, it was evident that the inferior medial limb of the right adrenal gland had unaffected adrenal cortex tissue that could be potentially preserved during resection.
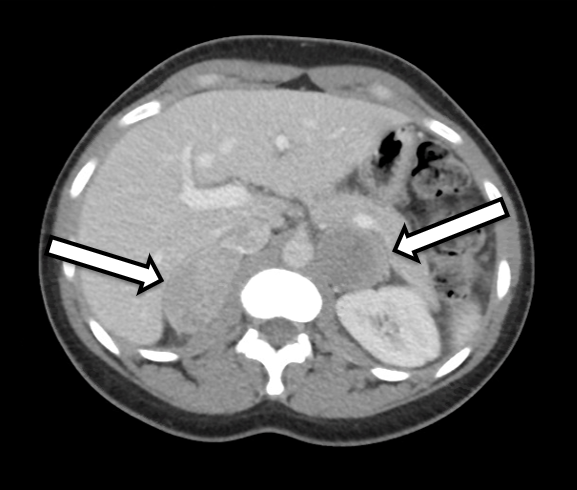
Figure 1. Transverse view of nodule within right thyroid lobe;
white arrows denote microcalcifications.
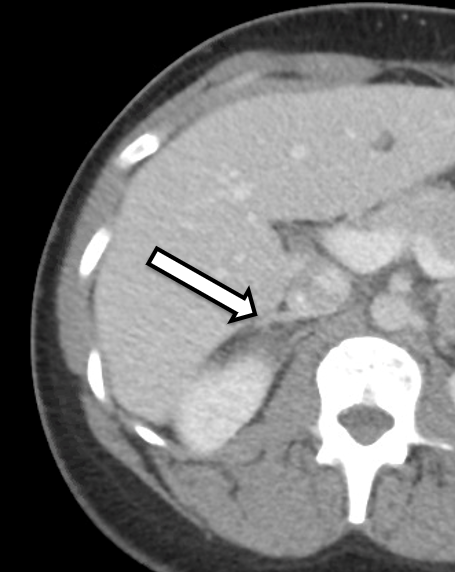
Figure 2. Enhanced view of CT of the abdomen demonstrating
normal adrenal cortex (arrow) of the right adrenal
gland that was preserved.
Pheochromocytomas originate from neural crest cells of the adrenal medulla and secrete excess amounts of catecholamines. The overall prevalence of pheochromocytomas has been estimated between 1:6500 and 1:2500, with an average age of onset between 40–50 years and a slightly higher prevalence in women. Most tumors are benign.6 Interestingly, there is no single pathological characteristic, including size, mitotic rate, or vascular or capsular invasion, that can accurately predict malignant potential, though various predictive algorithms have been created.7 Approximately 10–15% of tumors can present with and/or develop metastatic disease, indicative of malignant transformation.8 Disease-specific survival for malignant pheochromocytomas has been estimated to be approximately 70% at 5 years based on analysis of the Surveillance, Epidemiology, and End Results (SEER) database.9
Standard treatment for pheochromocytomas is surgical resection. Prior to the operation, the patient must undergo catecholamine blockade, which is usually performed using the nonselective alpha-receptor blocker phenoxybenzamine or a selective alpha-blocker such as doxazosin. Additional antihypertensive agents may be needed as well, including beta-blockers. However, beta-blockers should only be started after a patient has been placed on alpha-blockers to prevent a hypertensive crisis caused by an unopposed beta-receptor blockade. Furthermore, patients are chronically dehydrated and require preoperative fluid resuscitation.10
Patients afflicted with pheochromocytomas frequently suffer episodes of severe hypertension and other clinical manifestation of excessive catecholamine production, including palpitations, headaches, panic attacks, and diaphoresis.11 While blood pressure medications may provide partial relief, the only long-term, durable treatment is resection of the culprit lesion(s). Furthermore, those who continue without intervention are at risk of severe hypertensive crises, potentially leading to death.12 Therefore, patients with pheochromocytomas should seek surgical treatment expeditiously.
In patients presenting with bilateral pheochromocytomas, cortical-sparing adrenalectomy can prevent the occurrence of adrenal insufficiency while resecting the culprit tissue. Previous studies have shown that total adrenalectomy can be highly morbid. For example, in a series published by Lairmore et al. in which 43 patients underwent complete adrenalectomy for bilateral pheochromocytomas, 23% suffered episodes of adrenal insufficiency, and one patient died from an Addisonian crisis.13 Furthermore, patients who have undergone total adrenalectomy report poor quality of life and frequent hospitalizations related to adrenal insufficiency.14
Cortical-sparing adrenalectomy is an invaluable option for patients with genetic syndromes associated with pheochromocytomas. These syndromes include MEN2, VHL, and neurofibromatosis type 1 (NF1), as well as others. It is important to note that patients diagnosed with bilateral pheochromocytomas should be referred for genetic testing. Calcitonin testing may be a helpful adjunct to identify patients with MEN2, as genetic testing can take several months to be performed and properly interpreted. Approximately 40–80% of patients with either MEN2A or VHL will develop bilateral pheochromocytomas, and these tumors are usually benign.15 As such, cortical-sparing adrenalectomy can remove affected tissue, while leaving behind enough tissue to prevent adrenal insufficiency with minimal risk of recurrence.
The first case of cortical-sparing adrenalectomy was described by Irvin et al. in 1983.16 Since then, some institutions have reported success in performing cortical-sparing adrenalectomy through either open or minimally invasive approaches with fairly low recurrence rates, and importantly, low occurrence of adrenal insufficiency. 14 The use of PRA has been increasing as high-volume endocrine surgeons have implemented this technique. PRA was first described in 1995 and then further developed through the experience of Walz and his colleagues.1, 4, 17 Retrospective studies comparing PRA to LTA show decreased operative times, decreased blood loss, and no difference in long-term outcomes.
More recently, PRA is being utilized for cortical-sparing adrenalectomy as well. In a recent series, the experience over a 25-year period of performing cortical-sparing adrenalectomies for bilateral pheochromocytomas using the RPA approach was described. Sixty-six patients were operated on with a total of 101 adrenalectomies performed. Their mean operative time was 128 minutes for bilateral surgeries, and they reported only two major complications. They were able to perform a cortical-sparing operation in 89 of the cases and of those patients, 91% did not require steroids postoperatively. Only one patient had persistent disease, while no recurrences were reported.18 Patients should be cautioned that they might have some adrenal insufficiency following surgery. This is dependent on the size of the remnant adrenal tissue and the preservation of blood flow. Temporary adrenal insufficiency is managed in close consultation with endocrinology and appropriate laboratory testing.
The procedure is performed under general anesthesia with endotracheal intubation. Due to the hemodynamic alterations that can occur during surgery due to the tumor, an arterial line is placed for blood pressure monitoring, and the anesthesiologist administers vasoactive drugs as needed. A Foley catheter is placed to monitor urinary output. Depending on the degree of catecholamine elevation and other patient factors, a central venous line can be placed for additional venous access and monitoring of central venous pressure.
After induction of general anesthesia and endotracheal intubation, the patient is placed in a prone jackknife position with the hips bent at 90 degrees. A Cloward table with a Cloward Surgical Saddle is used to allow the abdomen to hang in a dependent fashion. The jackknife position and the Cloward Surgical Saddle open the retroperitoneal space to maximize exposure. All pressure points, including the face, arms, hips, and legs, are extensively padded. The iliac crest, the tips of the 11th and 12th ribs, and the edge of the paraspinous muscles are important landmarks marked by the surgeon. The initial incision is placed just inferior to the tip of the 12th rib. Scissors are used to sharply divide the soft tissue and enter the retroperitoneum. The surgeon’s finger is then used to bluntly clear space and guide placement of a 5-mm port medially and laterally, both angled at about 30 degrees and aimed toward the position of the adrenal gland. A 10-mm balloon port is then placed in the middle incision. The retroperitoneum is insufflated with CO2 through high-flow tubing to an insufflation pressure of 25 mmHg.
A 5-mm 30-degree scope is inserted in the 10-mm port, and a LigaSure device is used to create the retroperitoneal space. The dissection begins by identifying the paraspinous muscles medially, which is then followed by the identification of the kidney inferiorly. The camera is then typically moved to the medial port and the surgeon uses a LigaSure device and a bowel grasper through the lateral and central ports, respectively. Dissection continues over the superior pole of the kidney and along the paraspinal muscles medially, towards the direction of the adrenal gland. Exposure is facilitated in part by downward pressure on the kidney. As the adrenal gland is identified, the inferior extent of the gland and its relationship to the adrenal vein is determined. On the right, this dissection reveals the IVC, which the adrenal gland is dissected off of to reveal the adrenal vein. On the left, the adrenal vein originates from the left renal vein.
At this point, the precise relationship of the unaltered cortical adrenal tissue to the culprit tumor is determined. This is in part determined by a detailed evaluation of preoperative imaging in conjunction with intraoperative findings. Occasionally, intraoperative ultrasound may be useful. Once a suitable plane is identified, the pheochromocytoma is then divided from the normal adrenal tissue with a LigaSure device. The adrenal gland is a highly vascularized, so meticulous attention is given to hemostasis as the gland is transected. In this case, the inferior medial limb of the native right adrenal gland was suitable for preservation. If possible, the vein should be preserved. However, this not necessary, nor is it always feasible, given that there is additional venous drainage along the small adrenal arteries. During the current operation, the adrenal vein was found to be directly entering the tumor and as such it was divided with clips. At this point, the medial and lateral attachments of the tumor are taken down, leaving the superior attachment to allow the tumor to hang down and provide a superior site of counter-traction. Care is taken not to enter the peritoneal cavity during the lateral and cephalad dissections. Once the tumor has been circumferentially dissected, the superior attachments are taken, and the gland is removed from the retroperitoneal space with an Endocatch device. The 10-mm port is closed in layers, while the 5-mm port sites are closed only at the level of the skin.
Final pathology revealed a 5.2-cm right pheochromocytoma and a 5.6-cm left pheochromocytoma. Testing performed on postoperative day one demonstrated mildly decreased cortisol production. As such, the patient was temporarily placed on a low dose of oral steroids. The patient was discharged home on postoperative day two with excellent recovery when she was seen in the clinic two weeks following her operation, with a plan to wean off the low dose of prednisone.
Andrew frame, Cloward Surgical Saddle, LigaSure device, and Endocatch retrieval bag.
The authors have no disclosures.
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Citations
- Walz MK, Peitgen K, Hoermann R, Giebler RM, Mann K, Eigler FW. Posterior retroperitoneoscopy as a new minimally invasive approach for adrenalectomy: results of 30 adrenalectomies in 27 patients. World J Surg. 1996;20(7):769-774. doi:10.1007/s002689900117.
- Callender GG, Kennamer DL, Grubbs EG, Lee JE, Evans DB, Perrier ND. Posterior retroperitoneoscopic adrenalectomy. Adv Surg. 2009;43(1):147-157. doi:10.1016/j.yasu.2009.02.017.
- Perrier ND, Kennamer DL, Bao R, et al. Posterior retroperitoneoscopic adrenalectomy: preferred technique for removal of benign tumors and isolated metastases. Ann Surg. 2008;248(4):666-674. doi:10.1097/SLA.0b013e31818a1d2a.
- Walz MK, Peitgen K, Walz MV, et al. Posterior retroperitoneoscopic adrenalectomy: lessons learned within five years. World J Surg. 2001;25(6):728-734. doi:10.1007/s00268-001-0023-6.
- Lee JE, Curley SA, Gagel RF, Evans DB, Hickey RC. Cortical-sparing adrenalectomy for patients with bilateral pheochromocytoma. Surgery. 1996;120(6):1064-1071. doi:10.1016/S0039-6060(96)80056-0.
- Farrugia FA, Martikos G, Tzanetis P, et al. Pheochromocytoma, diagnosis and treatment: review of the literature. Endocr Regul. 2017;51(3):168-181. doi:10.1515/enr-2017-0018.
- Thompson LD. Pheochromocytoma of the Adrenal gland Scaled Score (PASS) to separate benign from malignant neoplasms: a clinicopathologic and immunophenotypic study of 100 cases. Am J Surg Pathol. 2002;26(5):551-566. doi:10.1097%2F00000478-200205000-00002.
- Pacak K, Wimalawansa SJ. Pheochromocytoma and paraganglioma. Endocr Pract. 2015;21(4):406-412. doi:10.4158/EP14481.RA.
- Goffredo P, Sosa JA, Roman SA. Malignant pheochromocytoma and paraganglioma: a population level analysis of long-term survival over two decades. J Surg Oncol. 2013;107(6):659-664. doi:10.1002/jso.23297.
- Li J, Yang CH. Improvement of preoperative management in patients with adrenal pheochromocytoma. Int J Clin Exp Med. 2014;7(12):5541-5546. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4307515.
- Chen H, Sippel RS, O'Dorisio MS, Vinik AI, Lloyd RV, Pacak K; North American Neuroendocrine Tumor Society (NANETS). The North American Neuroendocrine Tumor Society consensus guideline for the diagnosis and management of neuroendocrine tumors: pheochromocytoma, paraganglioma, and medullary thyroid cancer. Pancreas. 2010;39(6):775-783. doi:10.1097/MPA.0b013e3181ebb4f0.
- Sutton MG, Sheps SG, Lie JT. Prevalence of clinically unsuspected pheochromocytoma: review of a 50-year autopsy series. Mayo Clin Proc. 1981;56(6):354-360.
- Lairmore TC, Ball DW, Baylin SB, Wells SA Jr. Management of pheochromocytomas in patients with multiple endocrine neoplasia type 2 syndromes. Ann Surg. 1993;217(6):595-603. doi:10.1097/00000658-199306000-00001.
- Walz MK. Extent of adrenalectomy for adrenal neoplasm: cortical sparing (subtotal) versus total adrenalectomy. Surg Clin North Am. 2004;84(3):743-753. doi:10.1016/j.suc.2004.01.003.
- Renard J, Clerici T, Licker M, Triponez F. Pheochromocytoma and abdominal paraganglioma. J Visc Surg. 2011;148(6):e409-e416. doi:10.1016/j.jviscsurg.2011.07.003.
- Irvin GL 3rd, Fishman LM, Sher JA. Familial pheochromocytoma. Surgery. 1983;94(6):938-940. https://www.surgjournal.com/article/0039-6060(83)90403-8/fulltext.
- Mercan S, Seven R, Ozarmagan S, Tezelman S. Endoscopic retroperitoneal adrenalectomy. Surgery. 1995;118(6):1071-1076. doi:10.1016/S0039-6060(05)80116-3.
- Alesina PF, Hinrichs J, Meier B, Schmid KW, Neumann HP, Walz MK. Minimally invasive cortical-sparing surgery for bilateral pheochromocytomas. Langenbecks Arch Surg. 2012;397(2):233-238. doi:10.1007/s00423-011-0851-2.
Cite this article
Brown TC, Carling T. Bilateral posterior retroperitoneoscopic adrenalectomy with cortical sparing on right side. J Med Insight. 2021;2021(282). doi:10.24296/jomi/282.
Procedure Outline
Table of Contents
- Patient positioning
- Identification of external landmarks
- Marking
- Perform transverse incision just inferior to tip of the 12th rib
- Sharp entry into the retroperitoneum
- Use finger to manually bluntly create a small open retroperitoneal space
- Placement of 5-mm medial and lateral ports under manual guidance
- Place 10-mm balloon port and insufflate the retroperitoneum
- LigaSure to open the retroperitoneal space
- Identify the paraspinal muscles and the superior pole of the kidney
- Mobilize the adrenal gland inferiorly and retract the kidney downward
- Identify the IVF and mobilize the adrenal gland off the surface, medially and laterally
- Identify the adrenal vein, preserve if possible, otherwise clip and divide
- Divide the normal adrenal parenchyma from the culprit tumor
- Divide the superior attachments suspending the adrenal gland
- Place the gland in an Endocatch device and remove it from the retroperitoneum
- Inspect for hemostasis
- Close the fascia in the 10-mm port site
- Close the skin
Transcription
CHAPTER 1
I am Tobias Carling, I'm doing a bilateral retroperitoneoscopic posterior adrenalectomy. This is a patient that has pheochromocytoma bilaterally in the setting of MEN-2. Posterior retroperitoneoscopic adrenalectomy, we've been doing close to 10 years, here at Yale now, and we're one of the major centers in the world for this operation. The major advantage of doing a posterior retroperitoneoscopic adrenalectomy especially in the bilateral setting, is that it's much faster, quicker recovery, and the patients are faster back to normal activities. So, this patient is a 31-year-old female who was recently diagnosed with bilateral pheochromocytoma in the setting of MEN-2. As part of her workup, she also was diagnosed to have medullary thyroid cancer, which we'll be addressing in a couple of weeks. But because of her biochemically unequivocal pheochromocytoma syndrome, we elected to do the adrenalectomy first, so she has been on preoperative alpha blockade, and hemodynamically she's now ready for surgery. Studying her CAT Scan, as you can see here, is very important in this particular case because we want to try to achieve a cortical-sparing approach. And as you can see on the right side, you have the liver here and then you have the adrenal tumor on the right side here and on the left side - the aorta, the vena cava, and then the left kidney and the right kidney. And if you study very carefully this CT scan, you can see that almost a 5-cm pheochromocytoma on the right side and about 6-cm on the left side. But sitting right next to the vena cava, you actually have a little sliver of normal adrenal tissue, normal adrenal cortex, and that's why we will attempt to do a cortical-sparing resection on the right side. On the left side, however, pretty much the entire adrenal gland is replaced by this big, 6-cm pheochromocytoma. So a cortical-sparing resection is not possible on the left side. So that's why we started on the right side. So we started the operation on the right side doing a right posterior retroperitoneoscopic adrenalectomy. The ports are placed under direct palpation. We then identified the kidney. We do a fair amount of the dissection on the kidney without even seeing the tumor. But as the tumor is relatively large, you can easily see the tumor, which is sort of pale/gray compared to the normal adrenal cortex, which is more yellowish. And as you can see in the dissection, key landmarks on the right side is to identify the superior pole of the kidney, as well as the vena cava, and then in this particular case, the adrenal vein was sort of tucked underneath at the actual tumor, so that was ligated towards the very end of the operation. But as you could see, inferiorly and anteriorly there was a sliver of normal adrenal cortex as we predicted based on the CT scan. And this was able to be preserved, such that hopefully she'll have some cortisol production. We'll obviously measure that very carefully postoperatively to see whether she will need replacement or not. But once then the IVC as well as the kidney and behind the retroperitoneum, the liver had been identified, the dissection was quite straight forward and was done pretty much just with the LigaSure. So we then proceeded to the left side, which is done in a very similar fashion. The landmarks, again, is the superior pole of the kidney. As you can see, there was some superficial veins that we ligated with clips, but then the left adrenal vein as well as the phrenic vein, was easily identified and ligated as well, and again, the rest of the dissection was quite straight forward using just the LigaSure to divide all small, adrenal arteries to the left adrenal gland. The closure is relatively straight forward. The closure on the fascia for the big port, and then just a subcuticular closure for the skin.
CHAPTER 2
All right, so we're doing a bilateral adrenalectomy in a patient with MEN-2 that have bilateral pheochromocytoma, so we're going to attempt to do a cortical-sparing operation. The patient is 31 years old and was just recently diagnosed with both bilateral pheochromocytomas as well as medullary thyroid cancer.
CHAPTER 3
Okay. That's good. So I do a fair amount of the dissection here just bluntly, because I can sort of feel the tip of the kidney, right there. Okay.
Okay, that feels good. All right, we'll take the gas on.
Okay. Yep. All right, I'll take a LigaSure.
CHAPTER 4
Okay. Just show me muscle here. Okay, so that's the para - whoa, whoa, whoa, okay. Let's… I'll take a bowel grasper.
All right, so we got the kidney here. So, I'm just going to start mobilizing the superior pole of the kidney here. Can you just step down like… So we're mobilizing the superior pole of the kidney- so we do a fair amount of the operation without even seeing the adrenal at first. Okay. Okay. Okay. Come out and clean.
CHAPTER 5
Okay. All right, so come in here a little bit. So here is the pheochromocytoma, so I'm going to make sure I stay right on the peritoneal side here, because we want to see if we can save some cortex on this side, so - come back a little bit. That's adrenal cortex right there, which seems to be unaffected by the pheochromocytoma. It seems like the pheo ends right here. So if we could save this piece of normal adrenal cortex, that would be good. We're just going to mobilize a little bit more. Yeah. So I have the vena cava here, so - the vein is going to come in somewhere here, but because we want to save this piece of adrenal, we're going to eventually come across somewhere around here. But let's take a look. Over here, so come back now. And then, stay up here. Okay. Come back here. Okay, all right. Okay, so come back a little bit. Let's take a look. Can I have a suction for a second.
All right, so, I think - it feels like the tumor ends right here. So we're leaving this piece of adrenal tissue. Come back a little bit. Let's see… All right. Okay, come back a little bit. Cut - you're fighting me. So he's bleeding a little bit because we're coming through the adrenal parenchyma here. So I'm lifting the adrenal off the IVC here, so I'm taking care not to grab the actual pheochromocytoma or the - or the adrenal gland, but rather the fat next to it. Okay, that's good.
Now I'm going to grab that as high up as I can. And anesthesia, you guys are doing fine, right? Yeah. Because we're almost done with the left side here, so - right side, sorry. Okay, can you slide past that kidney at all? Just take a few steps down. Okay, so let's see what we got. So just come back a little bit. I'm just going to view it from below here. Okay. So that's normal adrenal there, and then, we got… I think that's the actual vein there. Okay. So we're going to ligate the vein here. You know, so the pheo is going right to the vein there, so we're not going to be able to leave any more adrenal cortex. So we have normal adrenal cortex here, just show that for a second. That looks, you know, very healthy. So, we're going to need a clip applier now.
So, her pressure might drop even a little bit lower now because we're ligating the right adrenal vein here. Uh, give me a… A LigaSure. All right, so come back and show me it. All right, are you happy with that? Do we want to put another clip on? Okay. Okay. Okay, good. All right, so we'll take a - Endo Catch.
CHAPTER 6
Okay. All right. All right, so we'll take lights on and gas off, all that stuff. All right, let's take a feel there, see if you can get it out. You might have to open it up a little bit. Okay. All right, so right adrenal. So call this right adrenal, cortical sparing. And then we'll take the ports back. I'm going to take another look.
CHAPTER 7
Okay, so that's the IVC, and then - so here's that - that's the right adrenal vein, right there. We were able to preserve some normal adrenal cortex, right here. And then the IVC looks good - no bleeding, no nothing. Okay.
CHAPTER 8
[No Dialogue.]
CHAPTER 9
All right, so we're going to start doing the left side. So again, doing a fair amount of dissection bluntly here, feeling for the paraspinous muscle.
And then I'll sort of angle this about 30 degrees up towards the adrenal, which will be up here. A port.
Okay. I'll take the camera. Gas on. Okay. All right, I'll take the LigaSure.
CHAPTER 10
Okay. So the first order of business is just to find your instruments and start creating the retroperitoneal space here.
So I've got the kidney here. Thank you. So, come back a little bit. Look down here. Thank you. Okay.
CHAPTER 11
All right, so we mobilized the kidney here. The tumor is sitting right up here. And the left adrenal vein is going to be down in this area. We'll get to it pretty soon. Okay. All right, so show me over here now. All right, so… Yep. So, I think that's the tip of it, come back a little bit. I just want to bring this even a little bit more like so. Okay. All right, come back a little bit. I don't love the exposure just yet. So the pancreatic tail is going to be right back here. That's a little bit of normal adrenal cortex there. Okay, come back. Come back a little bit. Okay. All right, come back. All right, just open this up a little bit more, so I can flip the kidney. Okay. Okay. These are the corners. They were underneath it right here. All right, just clean it for a second. When I was looking at the scan, and there's like pretty much tumor all the way to the vein here, so that's why the right was better to… To do the cortical sparing on. That's going to be the adrenal vein, right here. We're going to need a clip in the second. Thank you. All right, anesthesia, so we're ready to ligate the left adrenal vein here, so- so you might drop the pressure a little bit. Hopefully, not too much. All right, so, okay. Yeah. Okay, I'll take the clip. Okay. And I'm grabbing the adrenal vein with my grasper, which is a good place to grab because then I can mobilize the whole… Are we off the clip there - okay. All right. There might be another… No, I think that's just… Yeah, so this is the real vein, and also the phrenic vein is heading up right there. Yeah, so just follow me up here. Okay, so I can come back down. All right, so we'll take a clip again.
So we're - the previous one was just a superficial vein. This is the main adrenal vein we're clipping right now, so, just so you know. So here is obviously the kidney, here is the tumor, this is the left adrenal vein, that's the phrenic vein heading out there, so we're ligating it on the adrenal side of that. Okay, good. All right, so come back now. Now we're going to grab it as high as possible.
It's here. All right, good. Okay.
CHAPTER 12
All right, lights on. So the tumor is almost 5 cm, so we need to open up a little bit more. Thank you, Sam. That's good. Yep. Can I have a Kelly? There we go. All right, beautiful. So a little bit of normal cortex, but a typical pheochromocytoma.
CHAPTER 13
[No Dialogue.]
CHAPTER 14
So we just completed the bilateral posterior retroperitoneoscopic adrenalectomy. As you could see, the operation went really well, really no blood loss or any major difficulties. As you could see, we were able to save a small piece of normal adrenal cortex on the right side. Obviously, the key when you do a cortical-sparing adrenalectomy in the setting of MEN-2A is that you want to leave enough adrenal cortex such that the patient has cortisol production. But you don't want to leave too much or risk spilling pheochromocytoma tumor cells because then the patient can have a recurrence in the adrenal bed. So I think we were able to achieve that, where we just left a small piece of adrenal cortex on the IVC. The reason we did it on the right side as opposed to the left side is because we could predict based on the CT scan that it wouldn't be possible to save normal adrenal cortex on the left side because of the size of the tumor and the tumor encompassing the entire left adrenal gland. The patient did very well, hemodynamically, did not have any major swings in blood pressure and heart rate during the operation. And we always have a multidisciplinary pheochromocytoma team when we do this operation, with anesthesiologists that are used to this operation because there can be some challenges keeping up with the swings in the blood pressure primarily, but that was not a major issue in this particular case. Both sides went quite straightforward, and because of it being a pheochromocytoma, we'll routinely keep the patient in the ICU. I don't anticipate any issues in the blood pressure going forward, but that's a major reason to keep them in the ICU. If she does fabulously well, she may be able to go home tomorrow. If she needs to spend one more night in the hospital, that's fine as well. So postoperatively, as I mentioned, the patient will probably go home tomorrow or the next day. She'll have some soreness, because with the ports, as you can see, we do split some of the retroperitoneal muscles, so she'll have some soreness from that. A key obviously will be to measure her cortisol production, so we'll do what's called a cosyntropin stimulation test tomorrow morning to see if she has cortisol production. She may need a period of time of supplemental Prednisone, but that will be dependent on the lab tests tomorrow. Otherwise, people recover quite rapidly from this operation. Most people are back to normal activities in 1 to 2 weeks, and going forward, obviously, because of her MEN-2, she'll be surveilled the rest of her life, both for recurrence of pheochromocytoma, but also, as I mentioned, she also has a medullary thyroid cancer that I will operate on in a few weeks once she's, recovered from this operation.