
Squamous Cell Carcinoma Excision from Right Forearm with Split-Thickness Skin Graft from the Thigh
Main Text
Table of Contents
Skin is the largest organ by surface area of the body and is essential to prevent dehydration as the first barrier to infection, permit unrestricted movement, and provide a normal profile and appearance. A skin graft is a paper-thin piece of skin that has no fat or other body tissues attached and has been completely removed from its blood supply. Therefore, a skin graft can be transferred anywhere in the body as long as where placed, the so-called recipient site, does have a sufficient blood supply to nourish the skin until new blood vessels can grow into it within a short timeframe. Otherwise, if that does not occur, the graft will shrivel up and die. The downside even of a successful skin graft is the variable final color and inharmonious appearance of the skin, a tendency to contract possibly causing deformities especially limiting motion across joints, and similar healing issues at a second wound, that is the donor site of the graft itself. Nevertheless, this is a rapidly performed surgical procedure requiring but the simplest of instrumentation for the harvest of that graft that can then permit replacement of extensive skin deficiencies. In this video article, these virtues are displayed as a split-thickness skin graft is used to replace the skin missing following the removal of a large squamous cell skin cancer of the forearm.
This elderly woman presented with a long-standing, neglected, crusty, biopsy-proven squamous cell skin cancer of the top surface of her right forearm. Since larger than 2 cm in diameter, this would be a high-risk type of squamous cell skin cancer that has a high risk for metastasis or potential to spread to other parts of the body.1,2 As such, surgery would be the standard of care to try to remove all tumor cells by a wide excision into normal tissue about the tumor. The specimen obtained will always be reviewed later under the microscope to check all edges for any remaining tumor. If negative with no tumor seen, the chance of cure approaches 90% or more.2 If not removed at all, or if the edges still have tumor present, a squamous cell cancer will continue to grow where it began; but also can metastasize elsewhere, which could result in the death of the individual. Only for the extremely elderly or patients with other medical problems who would not tolerate the anesthesia for a major surgical operation would non-surgical treatment with radiation therapy be an alternate consideration.1,2
An operating room was used so that the patient would have a “twilight” sedation to make her pain free and comfortable.
To summarize the procedure in the video, an area extending about 10 mm into normal tissues all around the tumor of the right forearm was marked. This skin was cut around the tumor following those marks, and then down deep enough into the fatty tissues below to ensure that all tumor was removed. This left a large hole that could not be closed just by sewing together the surrounding skin, so another option had to be considered.
Because of her advanced age, her skin was very thin and fragile with minimal underlying fat tissue. Movement of that tissue with its blood supply intact, as what would be called a flap, was therefore considered impractical. Instead, to replace the missing skin, a skin graft was taken from her thigh as the best simple choice for her. Because no motorized dermatomes or skin harvesting machines were available to slice a thin layer of skin off her thigh much like a cheese slicer (i.e. Figure 1), instead a very sharp surgical knife was used to carve off the outer skin layer that would be the graft (i.e. Figure 2). Holes were pierced in the graft (i.e. Figure 3), which allows it to be spread apart to gain greater surface area dimensions; but also to permit drainage of any blood from the wound to come through them so that the graft is not lifted off the forearm before new blood vessels can grow into it to provide the necessary permanent blood supply. This step is called “pie-crusting,” analogous to that done by a baker to the top layer of the crust of a pie so that the steam created when baked can vent out through the holes and not explode the crust into pieces.
The harvested skin graft was stapled or sutured onto the forearm so that it would not move. A bulky dressing was next placed to stay on for a few days to prevent movement so that the graft would stick where fixed. The total time to obtain and place the skin graft was about a half hour with almost no blood loss, so the surgery was done as an out-patient allowing her to go home soon afterwards. The staples are customarily removed a week later as long as the graft seems to be “taking” by acquiring a pink color, which implies that circulation is being reestablished. Sometimes this can take several weeks to completely occur, until which time the graft could be grabbed and easily torn off the recipient site if one is not careful.
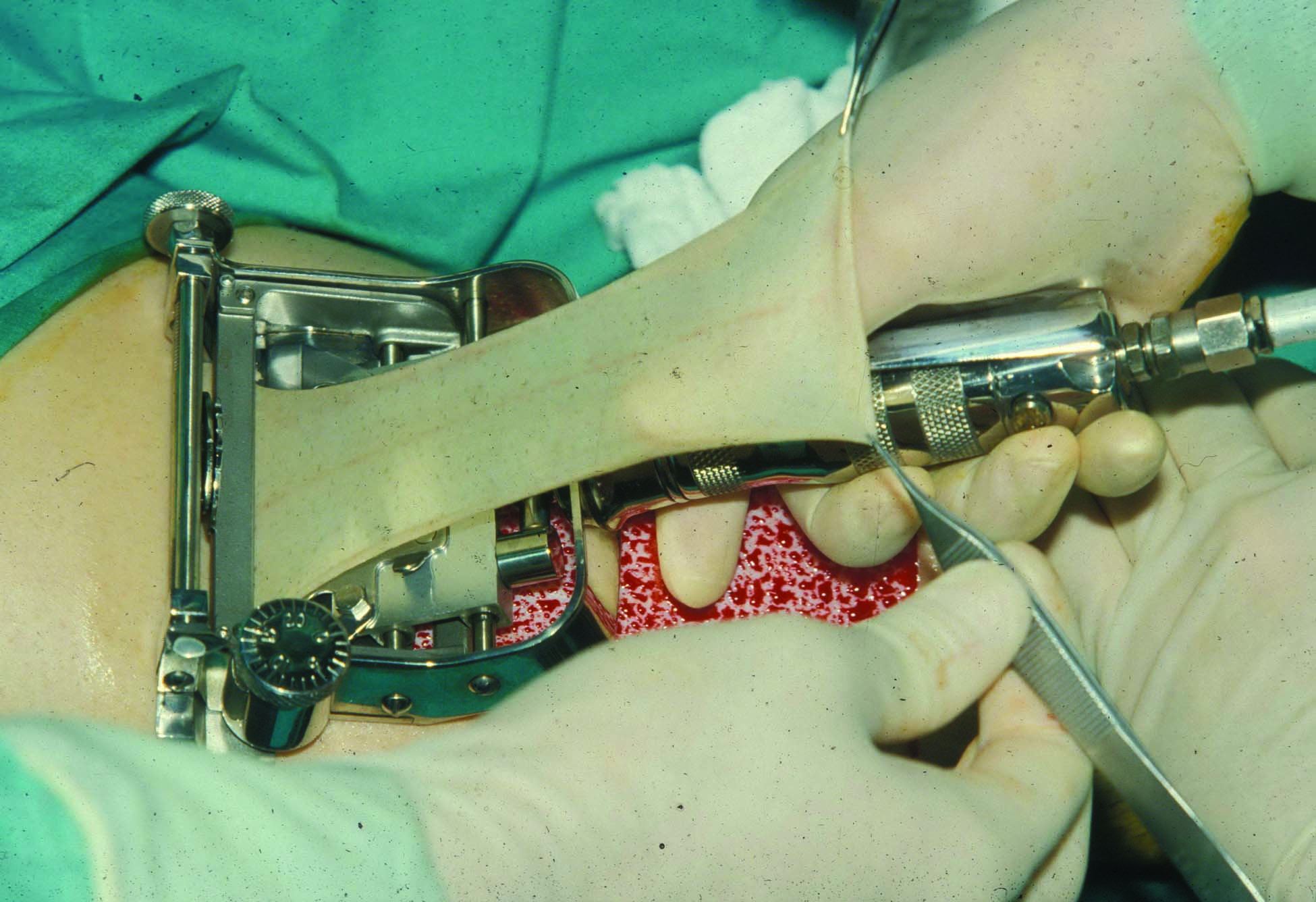
Figure 1. Motorized Brown dermatome allows rapid harvest of a split-thickness skin graft of predetermined thickness.
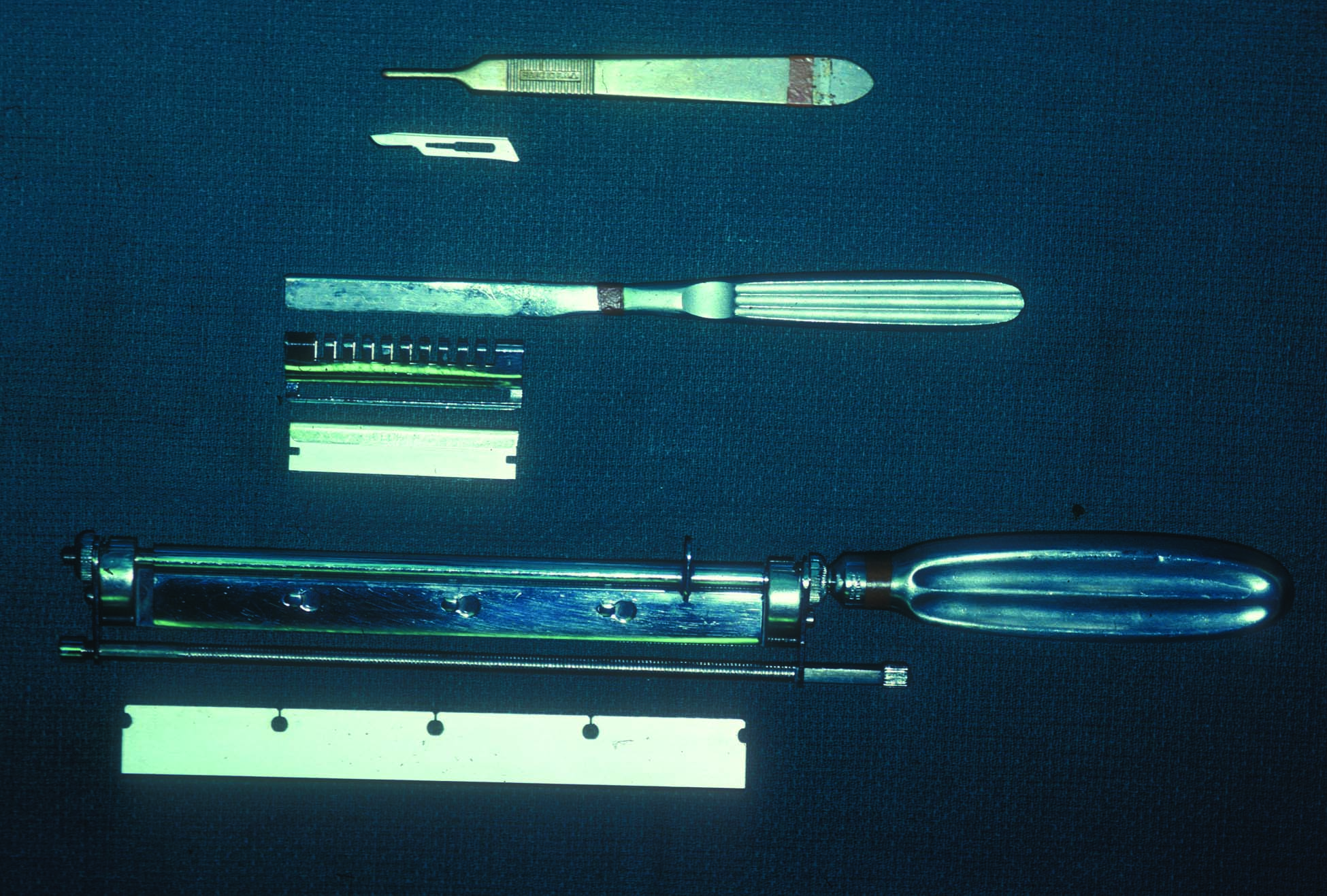
Figure 2. Special surgical knives and handles can be used for hand-harvesting a skin graft. From top to bottom these are a conventional scalpel, Goulian blade and handle, and Humby knife.
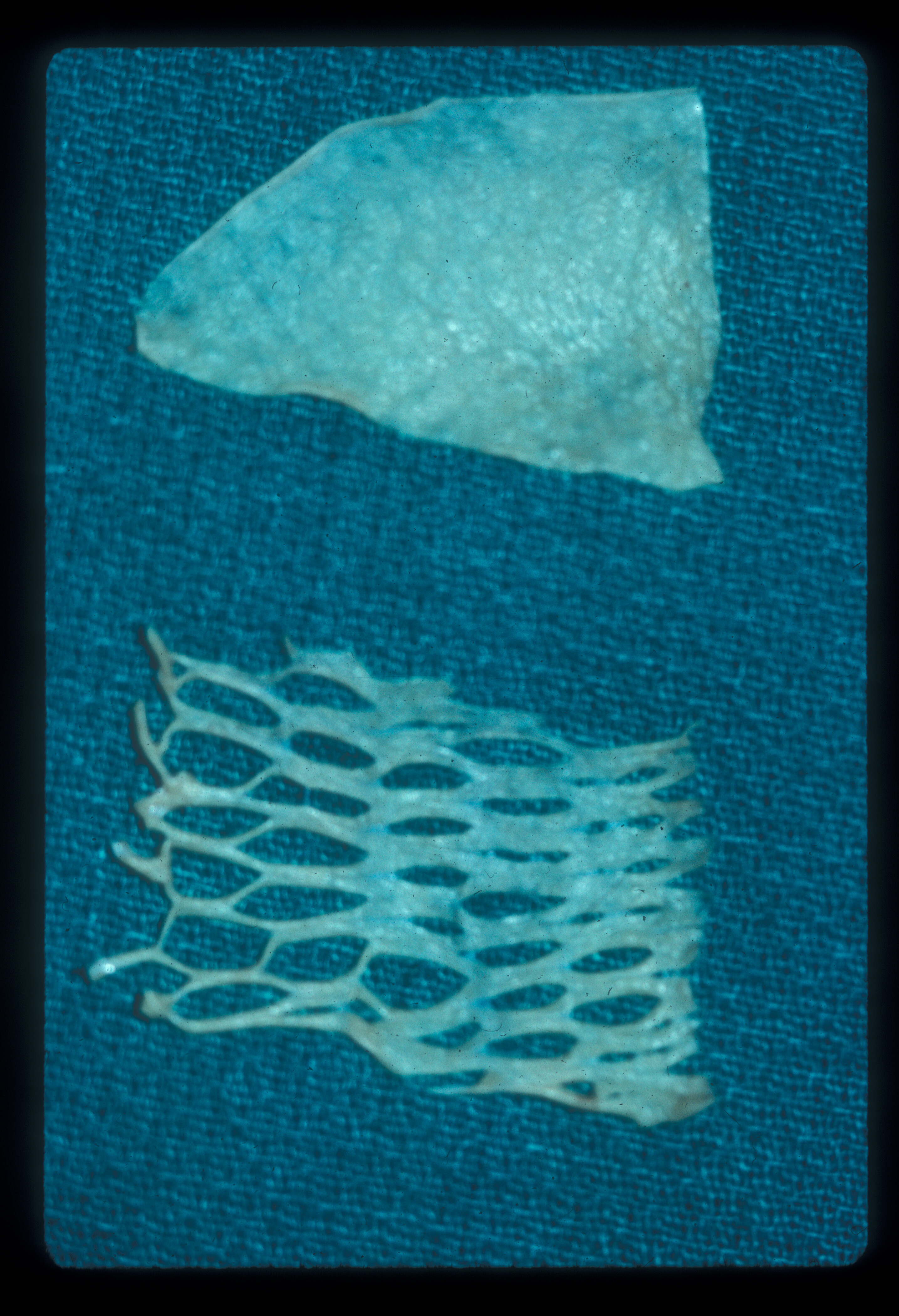
Figure 3. Sheet of harvested split-thickness skin graft (left) and meshed skin graft (right) with holes created for venting using a meshing machine or just a pair of scissors if necessary.
Squamous cell skin cancer is the second most common type of skin cancer.2 Basal cell skin cancer is 4-5 times more common, and the number of these two found every year exceeds the number of all other cancer types combined.1,3
There are many risks factors for causing squamous cell skin cancer that are similar to basal cell skin cancer such as fair skin, use of tanning beds, age over 40, and genetics; but far most common is the extent of sun exposure leading often to what is called an “actinic keratosis,” which is considered a premalignant lesion.2,3
The most characteristic appearance of a squamous cell skin cancer is a slightly raised pink plaque that often is scaly and can have open sores or ulcerations (i.e. Figure 4). High-risk lesions include large or deep lesions as in the presented case, rapidly growing lesions, or recurrent lesions that have grown back for whatever reason.1,2 Unlike basal cell skin cancers where there is little risk of metastasis or spread away from the origin of the lesion,3 high-risk squamous cell skin cancers have a rate of metastasis of about 30% and even those that are low risk have a 2–6% incidence of metastasis.1,2 If that occurs, death is a possible outcome that should be incentive enough for the patient to want whatever additional surgery is needed to ensure total tumor removal as soon as possible.4 Since more tissue is usually taken than must-be-removed to obtain a cure, more often than not, a skin graft as done here, or a flap, will be necessary to allow healing of the skin.
A simple way to get extra skin to cover any wound is to obtain and transfer a skin graft. Such use is well documented in Egyptian hieroglyphics, and even by the tile-maker’s caste in India centuries ago.5 When all the skin is removed from an area leaving the fat behind, this is called a full-thickness skin graft. This is most easily done with a surgical knife. If instead only the outer portion of the skin is separated, this would be called a split-thickness skin graft (i.e. Figure 2). The advantage of this option is that enough skin is left at the donor site that it will heal itself. Skin grafts may be taken from anywhere in the body, but an unappealing defect or scar will be left behind so it is best to use an inconspicuous location that is easily hidden especially by clothing (i.e. Figure 5). Since a skin graft has no blood supply, its survival relies on nutrients obtained from where it is placed, which must itself have a good blood supply. Thus, a skin graft sometimes cannot be used to cover for example exposed bone, and instead a flap that has tissues with their own blood supply would be preferable. Even when successful, a skin graft results in a suboptimal appearance (i.e. Figure 6), which might be devastating for a patient if used to cover any exposed regions such as the face.
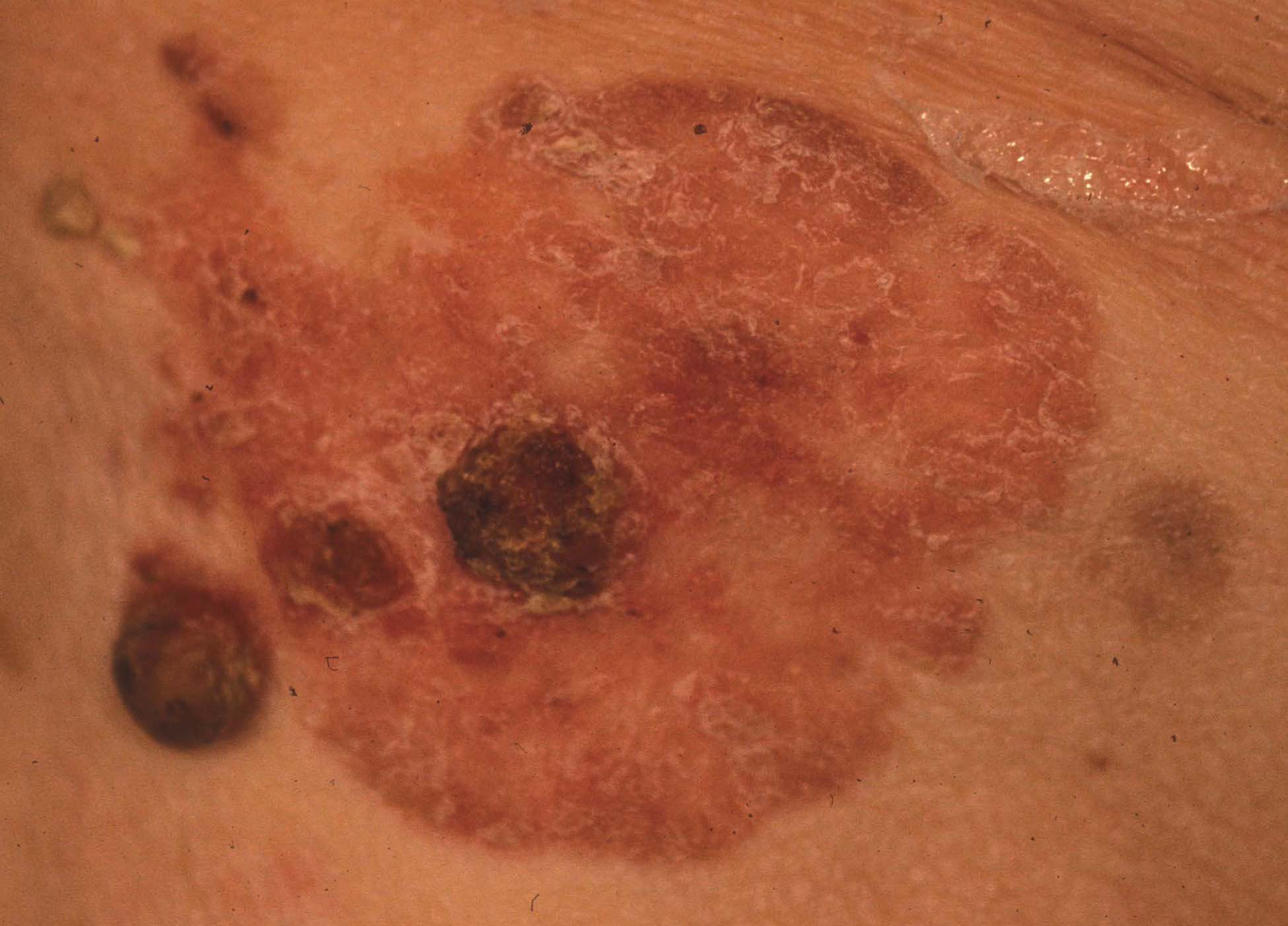
Figure 4. Common appearance of a squamous cell skin cancer as a pink plaque with a scaly or crusty surface.

Figure 5. Outline of a healed split-thickness skin graft donor site of the thigh, where the location is obvious due to the lack of skin pigmentation.
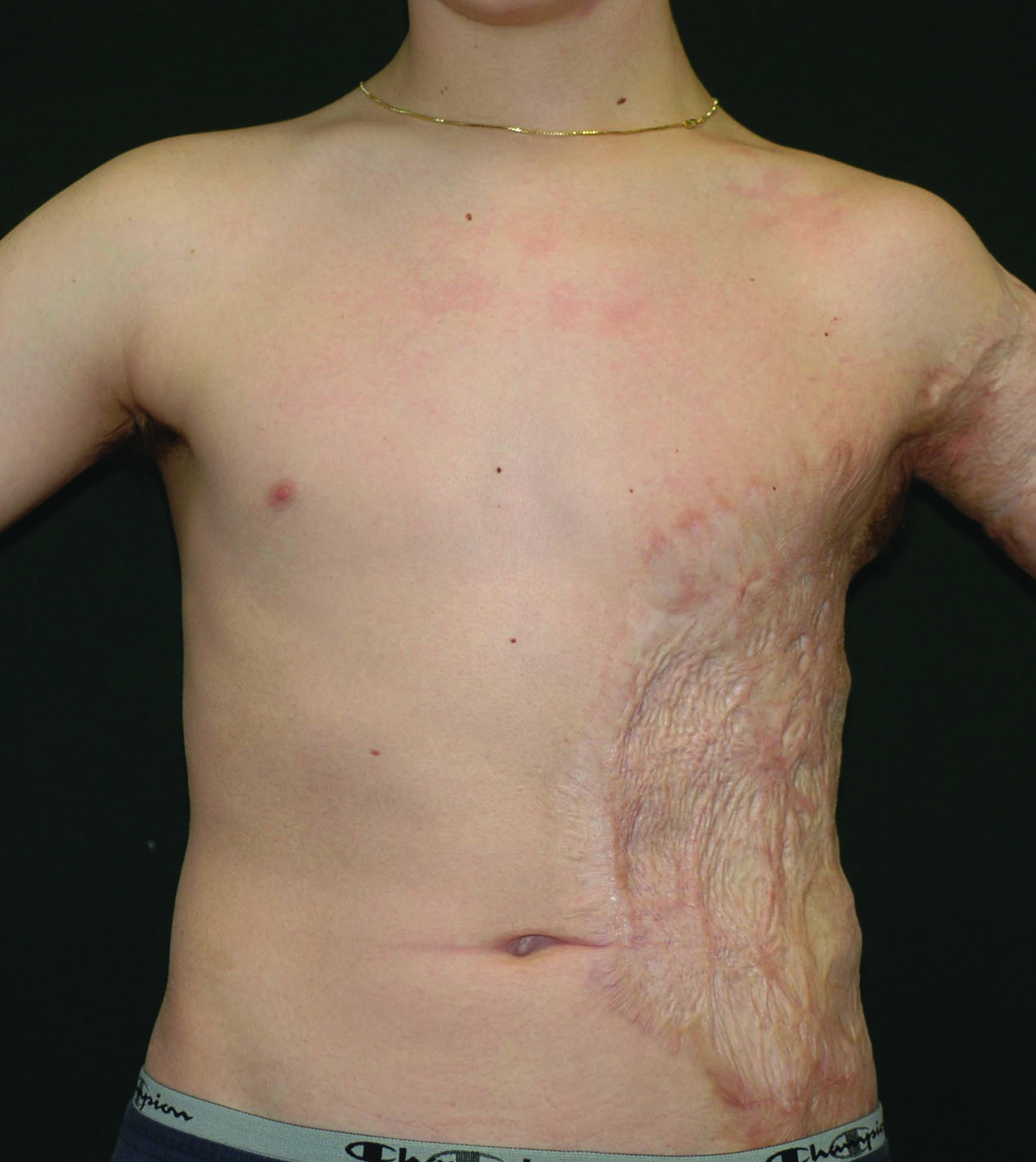
Figure 6. Healed skin grafts of the left flank and armpit of a young man who had been burned as a child. The grafts not only are of darker color but have an irregular contour and ridging due to significant scarring as well within and between grafts.
- Sharp surgical blades with special skin graft knife handles such as a Humby knife.
- Motorized dermatome for rapid, precise cutting of skin grafts.
- Scissors or skin mesher to create graft vent holes.
Nothing to disclose.
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Kate Mertz, Surgical Technician, from Bowmanstown, Pennsylvania, was the first assistant for all surgery.
Citations
-
Mendez BM, Thornton JF. Current Basal and Squamous Cell Skin Cancer Management. Plast Reconstr Surg. 2018 Sep;142(3):373e-387e. doi:10.1097/PRS.0000000000004696.
-
Rudolph R, Zelac DE. Squamous cell carcinoma of the skin. Plast Reconstr Surg. 2004 Nov;114(6):82e-94e. doi:10.1097/01.prs.0000138243.45735.8a.
- Gulleth Y, Goldberg N, Silverman RP, Gastman BR. What is the best surgical margin for a basal cell carcinoma: a meta-analysis of the literature. Plast Reconstr Surg. 2010;126(4):1222-1231. doi:10.1097/PRS.0b013e3181ea450d.
- An Introduction to Mohs Micrographic Surgery. American Society of Dermatologic Surgery.
Available at: https://www.youtube.com/watch?v=W5Paup_-S4A&feature=youtu.be. 2017. -
Hallock GG, Morris SF. Skin grafts and local flaps. Plast Reconstr Surg. 2011 Jan;127(1):5e-22e. doi:10.1097/PRS.0b013e3181fad46c.
Cite this article
Hallock GG. Squamous cell carcinoma excision from right forearm with split-thickness skin graft from the thigh. J Med Insight. 2024;2024(290.16). doi:10.24296/jomi/290.16.
Procedure Outline
Table of Contents
- Measuring and Marking
- Apply Mineral Oil
- Excise Graft
- Place Graft
- Staple Graft
Transcription
CHAPTER 1
Hi, this is Dr. Geoffrey Hallock. Today we're going to take care of a woman that has on her right dorsal forearm a squamous cell carcinoma. The cancer is about 3 x 4 cm in size, so it's fairly large. She does not have a lot of skin laxity in this area. To most simply close this after removal of the cancer is to do a skin graft. Specifically, a split-thickness skin graft. What we mean by that is that we're going to split the skin at our donor site, which will be her thigh, so that we leave enough behind so that the donor site will heal by itself taking only the epidermis and maybe a thin layer of dermis behind. I typically like to harvest these as about 13 one-thousandths of an inch in thickness. At the operating room that we were at we do not have a mechanical dermatome, which, of course, is the easiest way to harvest the skin. I'm going to rely on a time-useful method, it's proven itself, and that's with a Humby Knife. It's a very sharp knife, and we're going to take this and we're going to cut the skin of her thigh at the thickness that we want to do this. Now, I use the thigh as my donor site because it's fairly rigid. As a plastic surgeon I take it usually from the upper thigh so that underwear or shorts can hide the donor-site deformity because there's going to be one where the graft is harvested from. So I usually put, when I go to do the skin graft, I put some kind of lubricant like mineral oil on the area so that my knife will slide readily over the area I'm going to harvest the graft on as you will see. Once I have the graft of the size equal to the defect I'm going to cover, I will normally use a machine that will cut little holes in this, we call that a mesher. But again, in this case we did not have that available to us, so instead what we did is we cut little holes in the graft with scissors so essentially we form a meshing, but this time we're doing it by hand. This is a much more tedious way of doing it, but I think good enough to allow, in this case of this skin graft, it wasn't really the size of the graft that we needed but to make sure that the serum, or blood, or even some air pockets were underneath the graft, the graft would then lie flat on the area where we removed the skin cancer. That we call the recipient site, and it will be the source of nutrition to the graft for the first few days by what we call the plasma imbibition where the nutrients from the plasma will be in contact with the graft and that will keep it alive. In about 7 days the graft will start to get neovascularization from the underlying blood vessels as neovascularization occurs and that will then keep it alive. So we have to be careful for at least that period of time, usually, that there's not a lot of motion in the recipient area so the graft remains secure in that region. Once I put all the little holes in the grafts, starting on one side and then working to the other, I will then affix the graft to the edges of the recipient site. A very simple way, as we're going to use here, is to use a staple gun to do that. If you don't have access to a staple gun the alternative is to suture them in place as we used to do before we had staple guns. Once I have gotten all the sides of the graft fixed to the edges of the defect, the next step would be to put dressings on the graft. I like to use an antibiotic ointment impregnated mesh gauze, of some sort, that will easily slide off when I change the dressing and will not stick to it. On top of this I will put the bulky dressing of some sort, whatever you have available. I will then sew that in place around the graft rather than taping it to the forearm. First of all it's difficult to get tape to hold, but by sewing it in place there's enough pressure put on the graft, and you don't want to do this in excess, there's enough pressure, and we call this - a somewhat of a - what would be called a stent to hold the graft into position. Once that's taken care of attention should be directed to the donor site. You really don't want the donor site to dry out because you're relying on the epidermal buds, the hair follicles, sebaceous glands, sweat glands that have epidermis in them that you've not harvested with your split-thickness skin graft, and from that the epidermis will grow out and it will resurface the epidermal layer of your donor site. So you don't want that to dry out. So again, there are lots of ways of taking care of that. I find actually the best way to do that is to have some extra skin remnants that instead of throwing them away, just put them back on the donor site. The best recipient site actually is the donor site itself. So if you have any extra pieces of skin put them back in the center of your donor site and they can help spread out from the center to help cover the entire area. Actually that will heal faster than regeneration of the epidermis from the - from the epidermal buds.
CHAPTER 2
Okay, so here - you can see this ulcerating lesion here. If I mark it, I see - you know, I take off probably about 20 skin cancers a week, so I have a pretty good estimate what the margins are. I think that's just a keratosis. So here we go, here's our estimate of where the marks are. Again we're going to mark that at the 12-o'clock margin. Okay so we'll infiltrate this if we could. For me to get adequate margins on this cancer - see the size of this? This is about - I would say this is about 25 by 40 mm in size. So this is - this is extremely large. I have to take almost all of the skin of her forearm, and it doesn't have a lot of elasticity to it so I'm not going to be able to move that skin as I would for the keystone flap. So a keystone flap's not gonna be an option here. This is just too big. But a skin graft will be just perfectly fine here to fill this hole. That's what we're going to do now, we're going to show you what a graft is that has no blood supply but it's going to be adequate to close a defect this large. The first thing we're going to do is to infiltrate this with some local anesthetic that has epinephrine in it so we cut down the bleeding a little bit. And I think what we have here is bupivacaine which will also give some postoperative analgesia too. Okay, so while we're waiting for the - while we're waiting for the epinephrine to work let's show you how we're going to take the skin graft. So do we have our tool here to do that? So all this is is a big knife. I can turn the knob here and I adjust the thickness of what I'm going to harvest here. I don't - today we have mechanical dermatomes, but here we're going to use this one and we're going to shave the skin off the top taking the top layer. It is a split-thickness skin graft, leaving enough skin behind that that donor site where we take this from is going to survive. I use this - I don't use this to take skin grafts anymore, but I do use it to do like tangential excision of burns, for example, where you want to serially cut the burn down until it starts to bleed, and this is a good tool for doing that, but I have better tools for a skin graft. But this is what we're going to use today to try to show you how to do that to see what a skin graft is. And we'll come back and do that in a minute, but I want to see how big my hole is first so I know how much skin I have to take to fill the hole. We want to get all the roots out. As you can see, this is not deep. It moves - the skin moves, it's not going to be attached to the muscle or anything deep, so I know I can safely do this, and I'm doing it without a tourniquet. Because I don't need it really to do this. Okay.
CHAPTER 3
All right, so here we go. Kate's going to grab a suture then, and we'll mark that. Okay.
CHAPTER 4
Okay, I like to mark every specimen so that the pathologist has the orientation, and the part towards the head, we call that the cephalic margin, is the 12-o'clock margin. That's what I routinely mark. Okay scissors.
CHAPTER 5
All right, so here we go. This woman has an incredibly small amount of subcutaneous tissue, so I'm almost all the way down to the deep fascia. And amazingly almost no bleeding. We have a little bit but not much. All right there we go.
CHAPTER 6
Now you see, this hole is three times as big as the one we had on the chin. So - if I could do a keystone flap I would to avoid a skin graft, but she does not have enough skin to do this. Now it's - it's really important when you're doing a skin graft that you have no bleeding on the recipient site, this is the recipient site, this is where the graft's going to go. You must make sure you have no bleeding there because the blood underneath the graft will lift it up, and you will not get any new blood vessels growing into the graft. So it's very important here that you have no bleeding. It was not so important with the flap. I controlled it pretty well. But here it has to be very meticulous. Or the graft will just lift off and will not work.
CHAPTER 7
So that's - 4 x 5 - 4 x 5 cm - 4 x 5 cm that we need.
CHAPTER 8
I don't think so. No, I'm not worried about bleeding. Hmmm boy, yeah, this is going to be interesting. How do you choose like which part of the skin you're going to use for the graft? I can take the skin graft - I like to use - the reason I'm using the leg is it's pretty rigid so I'm taking that knife and I'm cutting against a structure that's not going to give very much. If I were taking it from your stomach, and I can do that, I can take a skin graft from anywhere, I can take it from your forehead, but most people don't want a mark where you took a skin graft on the forehead, so I like to take it from an area that's going to be cosmetically more acceptable like the upper-part of the thigh. The abdomen is a bad donor site, which I - in burn patients I will use that if that's the only place I can go, but there's so much - usually, there's a lot of fat there, it wiggles around to much to allow you to harvest it nicely even if with our mechanized dermatomes. So I need about that much skin to get this covered so I'm going to take a little bit extra. We're going to take some extra, and if I have extra skin graft, I'm going to put it right back on the donor site. This patient is 97 years old. 97 years old. And she's not going to heal very well. So we're going to do whatever we can to help her heal. So we'll get some mineral oil now. Did you put a little bit on the knife for me? Yes.
Okay. All right, we're just going to - apply some mineral oil so we have something that allows the knife to slip across.
About the thickness of a 15 blade. Okay, just pull this forward and down, and we're going to see if we can get this to work. Is that cutting? It's starting to. I don't know if this is going to be enough skin or not, but here we go. So all you need to take a skin graft is a knife. You don't need anything special. Okay. So you see how thin that is? It's actually not a bad graft. Just cover her defect. See how thin that is? And of course there's no blood supply to it. All right, so now we're going to take that - let's put something moist on the donor site so that doesn't dry out. You see the little fine bleeding here. We've left dermis there and epidermal appendages, and that will go on to allow that to heal. So now we're going to come back.
CHAPTER 9
I trained in North Carolina, and this is the North Carolina method of skin grafting. You're going to find everybody all over the world has different ways of doing it. See this shiny surface? The shiny surface - that's dermis. That's dermis. The shiny surface is dermis. That must go down, you want the epidermal side of the graft to be up, so don't make the mistake of putting the wrong side down. See the dull side? That's the epidermis side. Make sure that's the side that's up. So we're going to spread this out here, and see how we can cover this up. Now a machine that we do not have here with us in Honduras that we commonly use is called a mesher. And the mesher will take a piece of skin like this, and you can put holes in it, and I can spread this graft 6 times as wide, but we don't have that here so we have to use what we have. What I'm doing now is I'm - there's a tendency for the graft to roll under itself, dermis to dermis, so I have to unroll the skin. I do not want to have epidermis touching my recipient site so I'm unrolling it. See how much larger it really is. So once you have this all unrolled and put where you want it, the next step is how are you gonna hold it in place?
Many years ago when I was a resident what we would do is we would sew the graft in place. We'd sew it in place, but today we have staple guns, which are fast, and you can quickly do what would take us an hour to do with sutures. But I'm going to start off with the straight arrow scissors here if I could, please. The straight iris scissors. Remember I don't have a - I don't have a machine where I can put holes in this graft to spread it. And I like to put holes in for two reasons. One is so that the staples don't bunch the graft up, but number two is, we do what's called pie-crusting of the graft. I'll do this for almost every graft. When you put a pie in the oven, all the women know this, I don't, but we do what's called pie-crusting. You put a hole in the crust of the pie because as the pie heats up the gas expands, and if you don't put the holes in the gas will blow the crust off. Well the skin graft is a crust. In this case we don't have gas underneath the skin graft, but we do have blood and serum and stuff that will lift the graft up and off so it won't attach to the recipient bed and it will not get new blood vessels to keep it alive. They will not be able to grow in through the blood. So we pie-crust the graft also so that the blood has a way to get out from underneath the graft. And I don't have a machine to do this, so I'm just going to use scissors. And I'll take the staple gun. This is just like putting - just like putting the tar paper on the roof before you put the shingles down. You have a staple gun, put the tar paper down, that's all this is. You can see the staple coming out. So I see where the staple is. Remember I made that little hole, little pie crust in the graft. I'm going to grab it and I'm going to staple - I'm going to staple to the skin around the edge of the defect. All right, so when I put that in though, it moved the graft a little bit. Okay, so here we go. This is very tedious. I'll take the applicator, thank you. All right, notice that the skin is not exactly covering everything, but it's pretty close. The skin will grow across and it will cover the area where there is no skin. All right, I put a couple in just so that I wouldn't pull the skin graft off. And scissors, away we go. Okay, scissors. Are you stapling through the holes you made, or the skin? No, I'm going through the holes I made. If I staple into the graft it'll move the graft, and it won't lie - I want the graft to be - I want the graft to be - see how it wrinkles the graft up? I want that to be flat, you don't want - that's called tenting, you don't want that to happen. You want the graft to be flat so it can have total contact with the bed. Okay, scissors. Yeah, it's important that you have total contact everywhere. That's a good point to make. Okay, I'll take the scissors again. Okay, so we're almost there. Okay, so now I'm going to - now, I'm going to do that pie-crusting. What I'm doing now is I'm pie-crusting the graft, making lots of little holes. I'm really meshing the graft with my scissors, and I'll show you what this does here. It makes lots of little holes, lots of little pie crusts. See that little - you see air getting underneath the graft, we don't want air under the graft. I want nothing under the graft. So the machine would make these holes? Yes the machine would do this in 1 minute. What's taking me 10 minutes or more. Other applicator, please. Okay, so I made those little holes. I'm now going to advance this forward. See all the little holes? You can see them. You can see all the little holes that I pie crusted. Notice how it also helps me spread the graft over to cover - close the rest of the defect there. So that's pretty good. All right, so now I can go around the perimeter of my graft and I can finish - I'll do a little bit of this at a time. Okay, scissors. So I think you can start - you sort of see where I made all those little holes. I made all those little holes to pie-crust that. Those holes will close up by themselves. The skin will grow across and fill them in. In time. So I'm carefully going in those holes that I cut putting the staples in. I've now stapled my graft down, that's just some fat poking out. But I also like to put a second row of staples in - so that the graft does not slip - if one of my staples out here comes loose, the graft could slip. So I like to put a second row in. Are these going through the holes you pre-cut as well? These are the holes I pie-crusted. The pie-crust ones, okay. So you've spaced them out the size of the staples then? I did do that, I didn't say that did I? No, you did not. I did that so I can now... So you can do what you're doing now. I can now put some staples in where the pie crusts were. If I don't do it exactly right, see what happens there. Kate's going to take that one out. See what happened when I put that staple in? Yeah, it got bunched up. It got all bunched up there, I don't like that. That's not going to take well is it? So Kate's going to - take that one staple out with a hemostat. Okay, or use a scissors - or I can do it. Okay. Okay, be careful that you don't lift the graft off and mess everything up. Okay. All right, now we've got it flat again, okay? So I was not happy with that. I want it down flat. Okay. Let's see if I can do it right this time, okay? That's a little better. Don't be afraid to redo something if you're not happy. You see, that came out perfect, okay? If you're not happy, don't be afraid to redo it. I don't think I'm going to have any extra skin to put back on. All right, so that's not bad. Let's just show people how we dress this, okay? Just give us a piece of Xeroform. All right, so we're done here.
CHAPTER 10
Now I'm going to show you how I put my dressings on. So I don't - I don't want the graft to move on the arm because every time it moves the new blood vessels can't grow into from below, and I also want to put pressure on it - on the graft so that it's stuck to the recipient site, as well as possible, that's important I think. And they call this a stent if it's in the mouth. And so what I'm doing is like a stent to hold the dressing in place. It puts pressure on it to hold it in place. Okay, so I'm going to estimate the size of my defect. This is just a piece of Xeroform. You don't have to use Xeroform, you can use any kind of minimally-adherent gauze with petroleum jelly on it, or you put a Band-Aid on it. And that looks good, okay. And then I'll just take a 4 x 4 sponge. Just as a regular - they call it "gasa" here, just a regular sponge, that I fluff up. And I'll fill that into the hole, and we have a compress? Yeah, that's a little bit thick, but this is a nice, soft dressing. And every operating room has them. And there we have it, that's good. And I'm going to sew the dressing on. That's - you say boy that's weird, isn't it? But that's what I do because it provides some extra - extra - protection for the graft, it also puts pressure on it so that it doesn't move. Surgeons tend to be very practical people, so - how long do you keep the dressing on is the question that was asked. It depends on where you are in the world, what you're doing, what kind of backup you have. I will normally take this dressing off in 48 hours. Today is Thursday, 48 hours will be "sabado", Saturday. And we're going to wait until Monday to take it off because nobody will be here on sabado. We're going to wait until Monday. And that's not going to hurt at all. That means that the patient will have one less dressing change probably. Because once I take it off, I usually change the dressings every 2 days to see how the graft's doing. And that pretty well secures it - that the dressing's not going to fall off. But I will go in between here just to - because I want more pressure. If you just have the 4 corners, there's not going to be a lot of pressure on it so I want a lot of pressure holding that graft so it doesn't move. And - as far as the donor site goes, I also will put a dressing on that does not stick there. If I had had extra skin here I would have taken it and put it back on the donor site to help that heal, but I had no extra skin. I barely had enough to cover the hole I had. And most people don't do that, but I do. The best recipient site for a skin graft is the donor site. If that makes any sense because that's where it came from. This recipient site here is not bad, the patient's going to do well I'm sure, as long as she doesn't rub the graft on. So I usually wait, after I do a graft, I'll take the staples out in maybe 6 days. After about 2 weeks the patient can wash the graft and go about their normal existence, usually if it takes well. So, but up until 2 weeks all I have to do is take my forceps and I can just pull the graft right off. It takes 2 weeks really to be stuck, so you can't do that easily. Okay Kate, so if you could cut that suture please for me. And Kate is now going to show you how we treat the donor site. Oh, that's all we have? Okay we're going to use what we have available and we're just going to cover that up with a gauze, sponge on it. I like not to overlap that, but she did, but we use what we have. So this fine mesh gauze is going to allow the blood to come through it into the dressing. This is not the optimal donor-site dressing, but this is what we have.
CHAPTER 11
In this case we just put an antibiotic-impregnated gauze over the donor site and then a light dressing. I usually take that off in 48 hours, sometimes in 6 days, so that there's some healing there because that's going to be very painful. As a matter of fact that's where all the pain will be for the patient is in the donor site itself. And then, because it's messy, then this is not the optimal way to treat the donor site, but because it's messy we usually have the patient take a hair dryer, this is somewhat of an old fashioned way of handling the donor site, but it keeps the patient's clothing and bed linens from getting dirty from the donor site. The recipient site, most often in 48 hours I remove the dressing very carefully from that. I inspect the skin graft to make sure that it's adhering to the recipient site, there's no problems. I will put pressure on the graft itself as I'm peeling the dressing off, to ensure I don't accidentally lift the graft up and so it remains adherent to the recipient area. I then redress that with a non-stick dressing of some sort, come back in about 6 days again. By then the graft is stuck enough, and you can probably remove safely the staples from the area. I then keep a dressing on of some sort that doesn't stick. Most commonly, it depends again on the age of the patient, their health, what the defect is, where it is in the body, how long you're going to keep dressings on until it is healed, that's up to the discretion of the surgeon of course. It's really important that the patient understands that a graft, as opposed to a flap, has no blood supply. It relies on the recipient site to survive, so they have to be very careful they don't sheer the graft or move it in any way so that it doesn't - lose the ability for the new blood vessels to grow into it to keep it alive. Usually, depending again on what part of the body, face maybe in 7 days the graft's going to be revascularized. In the lower extremity, maybe 2 weeks before you have adequate take of the graft, sometimes even longer.